
Alcoholic liver disease: Morphology, Clinical features & Complications
ALCOHOLIC STEATOSIS- FATTY LIVER
Gross:
Size- enlarged
Capsule: stretched
Margins: round
Color: yellowish gray
The cut section: yellowish gray greasy
Microscopy: In the initial stages, the neutral fat is dposited around the nucleus. These fat in stained sections are seen as micro vescicles with clear content ( as the fat in these vescicles are cleared during the processing of tissue) This stage is microvesicular fatty change. over time, the vescicles enlarge to become macrovescicular and thereby pushing the nucelus to the periphery and finally some of these vescicles fuse to form fatty cysts. Rupture of the cysts may lead to inflammatory reaction around them.

Fat stains: Can be demonstrated in fresh unfixed tissue by frozen section
The following stains can be used and the color taken by the fat (in frozen section) are as follows
a. Sudan III– yellow
b. Sudan IV( Scarlet red)- Orange
c. Oil red O – Red
d. Osmic acid – Black
e. Sudan Black B – Black
ALCOHOLIC HEPATITIS
GROSS: Liver enlarged as in steatosis. May be more firm due to beginning of fibrosis
MICROSCOPY
The following features are seen.
a. Hepatocyte swelling: Ballooning – Swollen hepatocytes with clear cytoplasm
b. Hepatocyte degeneration: Aggregation of cytokeratin – seen as Eosinophilic cytoplasmic inclusions called as Mallory bodies named after Frank Burr Mallory, an Americal Pathologist.
c. Inflammation: Plenty of neutrophils around the necrotic hepatocyte. Lymphocytes can also be seen.
d. Fibrosis: early stage of fibrosis- is usually Perisinusoidal/ pericerllular, Begins in zone 3. This pericellular fibrosis is referred to as chickenwire fibrosis.
ALCOHOLIC CIRRHOSIS
GROSS
Initially , the liver is enlarged,yelloish and fatty and show nodules less than 3 mm in diameter. This is referreed to as Micronodular cirrhosis.
After many years. these nodules coalsce and enlarge to form macronodules( nodules >3mm in diameter). The liver appears Brown, Non-fatty and Shrunken.
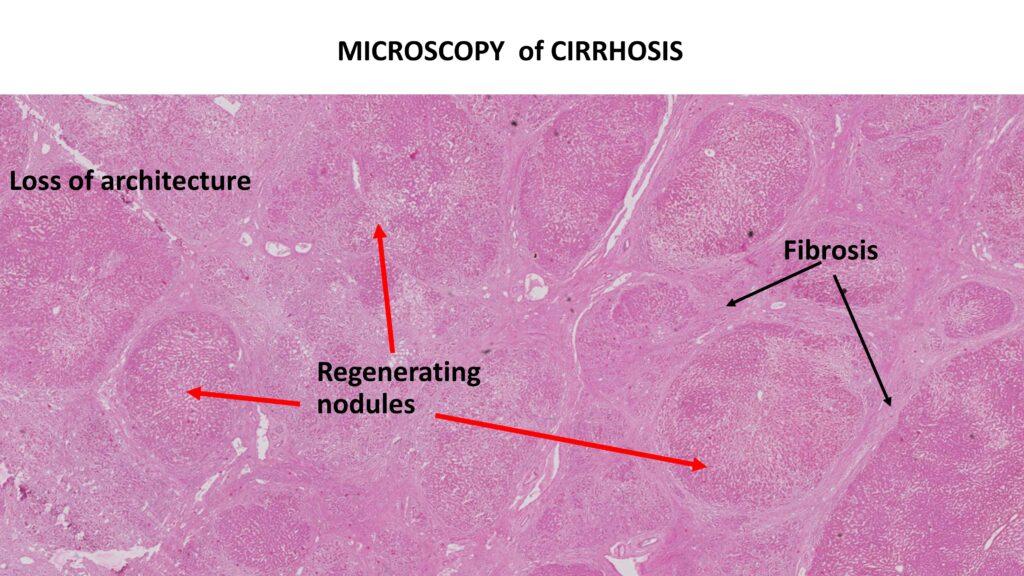
MICROSCOPY
There is Loss of architecture. Regenerating nodules are seen separated by bands of fibrosis. Masson’s trichrome stain helps in demonstration of fibrosis.
CLINICAL FEATURES
Alcoholic steatosis: hepatomegaly, with mild elevation of serum bilirubin and alkaline phosphatase levels.
Alcoholic hepatitis : appear acutely, usually following a bout of heavy drinking. they have malaise, anorexia, upper abdominal discomfort, and tender hepatomegaly. hyperbilirubinemia, elevated serum
aminotransferases and alkaline phosphatase are the lab features.
Alcoholic Cirrhosis: Nonspecific initially. Anorexia, weight loss , weakness. Hepatic failure in advanced disease.
Elevated serum aminotransferases, hyperbilirubinemia, variable elevation of serum alkaline phosphatase, hypoproteinemia (globulins, albumin, and clotting factors), and anemia are the lab features.
COMPLICATIONS:
Portal hypertension: Elevation of hepatic venous pressure above 7mmhg which further leads to
a. ASCITIS
b. PORTOSYSTEMIC VENOUS SHUNTS
c. CONGESTIVE SPLENOMEGALY &
d. HEPATIC ENCEPHALOPATHY
Causes of death in In advanced alcoholic liver disease includes
1. hepatic coma,
2. massive gastrointestinal hemorrhage,
3. intercurrent infection (to which these patients are predisposed),
4. hepatorenal syndrome (often following a bout of alcoholic hepatitis), and
5. hepatocellular carcinoma
Click below to watch the video tutorial

{kind=link}