
Acute Post-Streptococcal Glomerulonephritis
Overview
Acute post-streptococcal glomerulonephritis belongs to a group of diseases known as proliferative glomerular nephritis.
These diseases are characterized by diffuse proliferation of glomerular cells and infiltration of leukocytes, particularly neutrophils. They are typically caused by immune complexes formed in response to antigens, which can be either exogenous or endogenous.
Immune Complex Formation
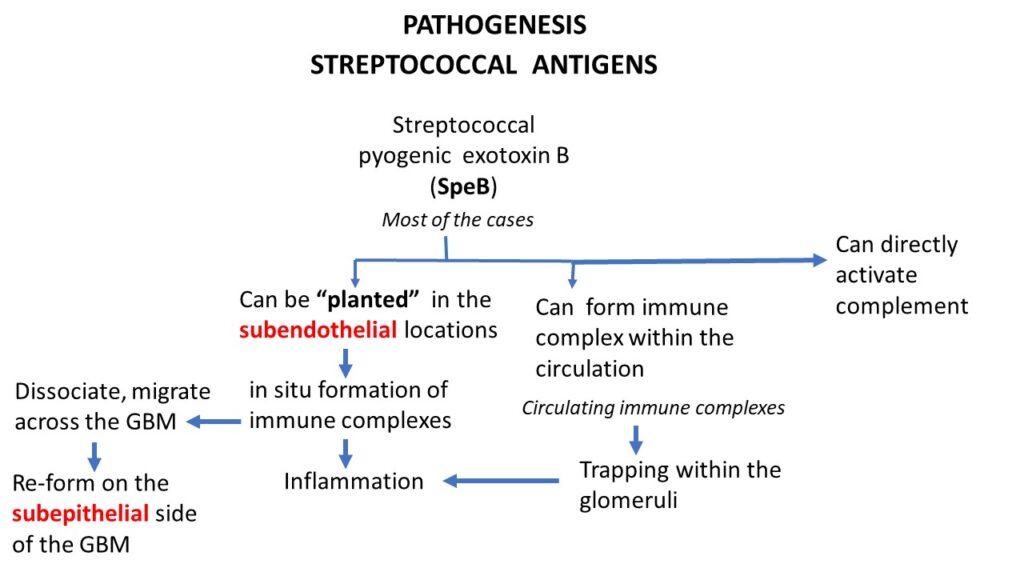
Immune complexes play a crucial role in the pathogenesis of glomerular injury. In acute post-streptococcal glomerulonephritis, the immune complexes are formed in response to the streptococcal antigen, specifically the streptococcal pyogenic exotoxin B. These immune complexes can form inside the glomeruli (subendothelial) or circulate in the blood and get trapped in the glomeruli. They can also directly activate complement, leading to inflammation.
Causative Organism
The causative organism for acute post-streptococcal glomerulonephritis is group A beta-hemolytic streptococci, specifically nephritogenic strains of types 12, 4, and 1. These strains affect the kidneys and result in the development of glomerulonephritis.
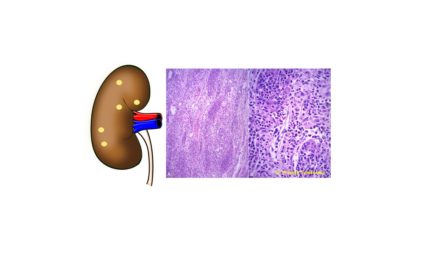
Morphology
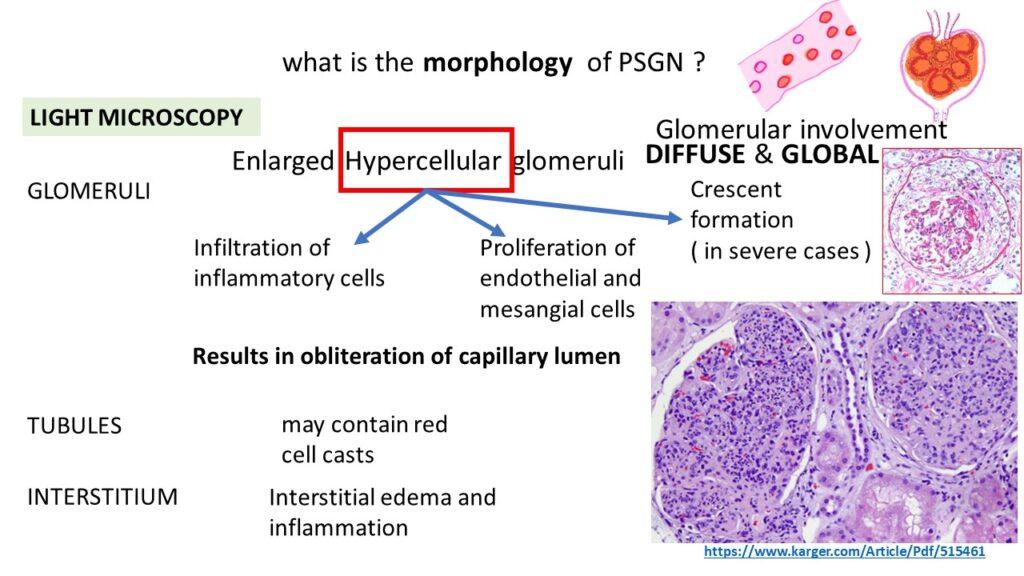
Under light microscopy, the glomerular involvement in acute post-streptococcal glomerulonephritis is diffuse and global. This means that more than 50% of the glomeruli are involved, and within each glomerulus, the entire structure is affected. The glomeruli appear enlarged and hypercellular due to inflammatory cell infiltration and proliferation of endothelial and mesangial cells. In advanced cases, crescents may form, leading to the obliteration of capillary lumens and reduced glomerular filtration rate.
Immunofluorescence and Electron Microscopy
Immunofluorescence microscopy reveals granular deposits of immunoglobulin G (IgG), complement component C3, and occasionally immunoglobulin M (IgM). These deposits are located in the subendothelial or subepithelial spaces and appear granular. Electron microscopy shows electron-dense deposits in the subepithelial, subendothelial, or mesangial regions, and sometimes within the glomerular basement membrane. The characteristic feature is the presence of subepithelial deposits.
Clinical Features of Post-Streptococcal Glomerulonephritis
Typical Case Scenario
A typical case of post-streptococcal glomerulonephritis involves a young child who had a previous sore throat or skin infection. After a period of one to two weeks of asymptomatic period, the child suddenly presents with the following clinical features:
Malaise
High-grade fever
Nausea
Oliguria
Hematuria (smoky or cola-colored urine)
Periorbital edema (due to mild proteinuria)
Mild to moderate hypertension
Periorbital Edema
Periorbital edema, the swelling around the eyes, is a common manifestation in post-streptococcal glomerulonephritis. This occurs because the periorbital area has an abundance of lymphatics, which can be affected by interstitial changes caused by the disease process.
Laboratory Findings
In terms of laboratory findings, the following can be observed:
Urine examination: Hematuria and proteinuria
Serum examination: Elevated levels of anti-streptococcal antibody titers (ASO titers) and anti-DNase B antibodies, decline in serum concentration of complement component C3, and other components
Treatment
The primary treatment for post-streptococcal glomerulonephritis is supportive care, focusing on managing blood pressure. This can be achieved through:
Diuretic administration
Salt and fluid restriction
Antibiotics do not have a significant role in the treatment, unless there is evidence of ongoing streptococcal infection or suspicion of residual infection.
Prognosis
The prognosis of post-streptococcal glomerulonephritis depends on the age group:
Children: In the majority of cases (95%), children recover renal function with conservative therapy. Less than 1% of cases develop rapidly progressive glomerulonephritis, while the rest may experience slow progression to chronic glomerulonephritis.
Adults: Adults may have persistent hematuria, proteinuria, and hypertension. Progression to rapidly progressive glomerulonephritis or chronic glomerulonephritis is observed in a significant number of cases.
Click here to watch the video tutorial on acute post streptococcal glomerulonephritis
“Need the notes? Download the PDF“
{kind=link}