
Carcinoma oesophagus – Squamous cell carcinoma
The malignant tumours of oesophagus include squamous cell carcinoma and adenocarcinoma. Of these squamous cell carcinoma is more common.
Squamous cell carcinoma occurs in individuals above 45 years of age, with a male predominance.
The incidence of oesophageal carcinoma varies with the geography and is particularly more common in rural and low-income countries.
A very high incidence is observed in western Kenya due to the tradition of consumption of fermented milk (Termed Mursik) which contains acetaldehyde which is a carcinogen.
Risk factors include
Alcohol
Tobacco use
Poverty
Chemical injuries to oesophagus
Achalasia
Diets deficient in fibres
Plummer-Vinson syndrome
Consumption of hot beverages frequently
Previous history of radiation to mediastinum
HPV infection
Molecular pathogenesis
Recurrent abnormalities include: Amplification of SOX2
Overexpression of cyclin D1
Loss-of-function mutations in TP53, CDH1 and NOTCH1
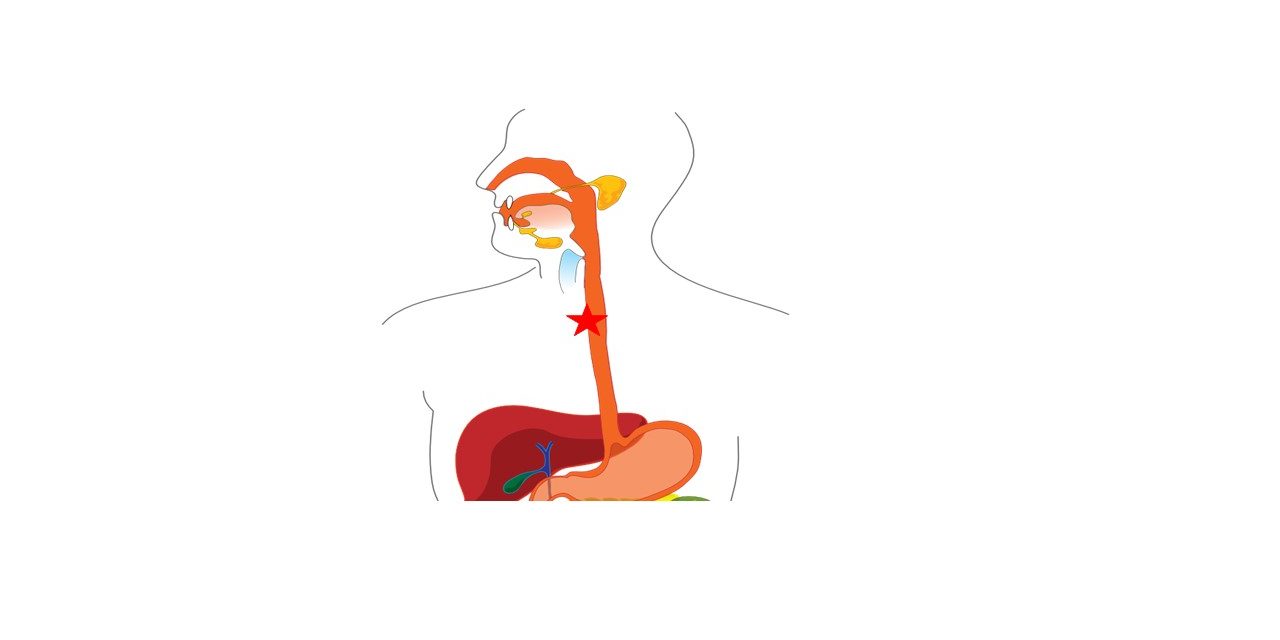
Morphology – Gross
Most commonly involve the middle third of oesophagus.
Early lesions can appear as grey-white plaques.
It can present as polypoid or proliferative exophytic mass projecting into the lumen. Large tumours can cause obstruction.
They can also present as ulcerated growths or diffusely infiltrating lesions with wall thickening.
They can invade the surrounding structures like aorta, mediastinum, pericardium, pleura or lungs.

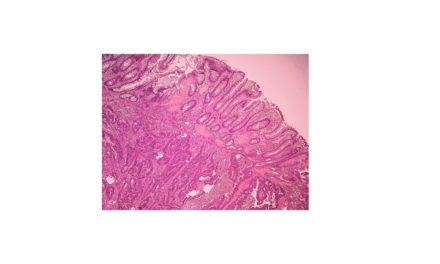
Morphology – Microscopy
Squamous cell carcinoma begins as dysplasia – intraepithelial/ insitu carcinoma i.e tumour confined to the epithelial lining without the breach through the basement membrane. Once the basement membrane is breached, it becomes invasive carcinoma.
The tumors can be well-differentiated, moderately-differentiated or poorly-differentiated depending on the degree of resemblance to the benign squamous cell and amount of keratin pearl formation.
Tumor cell are polygonal with enlarged, hyperchromatic nucleus and moderate to abundant well-defined, eosinophilic cytoplasm. Nuclear pleomorphism and tumor giant cells can be seen. Intercellular bridges, individual cell keratinization and keratin pearl formation can be seen. Mitotic activity depends on grade of tumor.


Rare variants : squamous cell carcinoma, spindle cell carcinoma, and basaloid squamous cell carcinoma
The lymphatic network of the esophagus is very rich and promote metastases, as well as circumferential and longitudinal spread.
The sites of lymph node metastases vary with the location of primary tumor
-upper third of the esophagus favor cervical lymph nodes;
-middle third favor mediastinal,paratracheal, and tracheobronchial nodes;
– lower third spread to gastric and celiac nodes

{kind=link}