
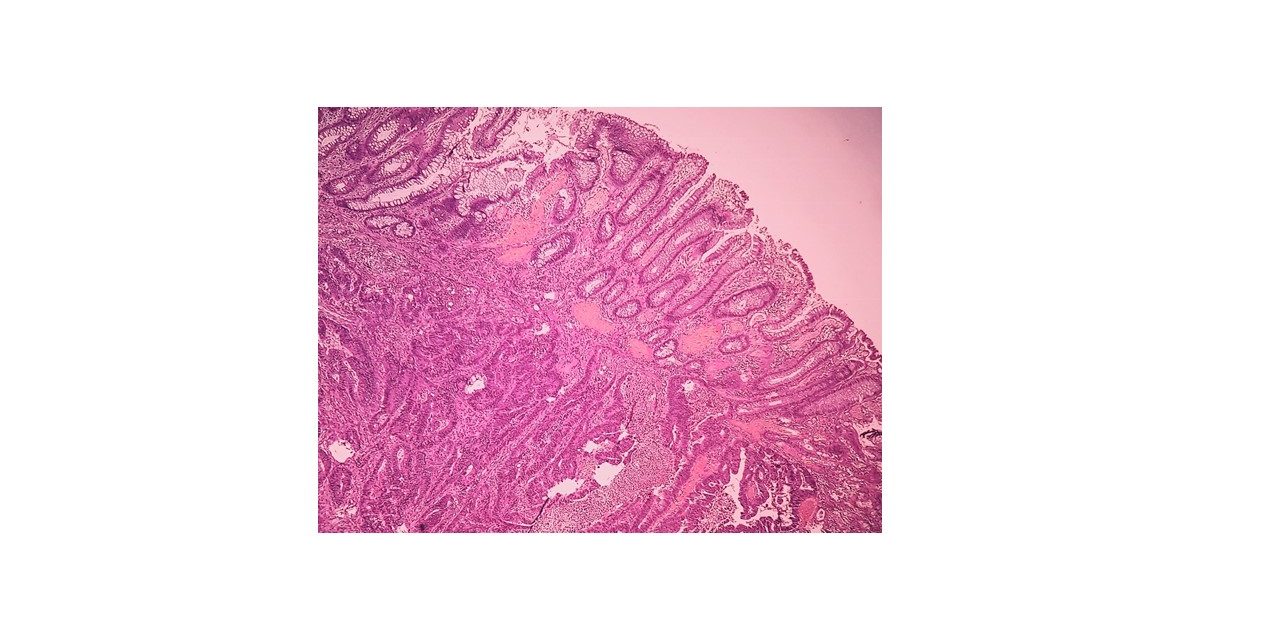
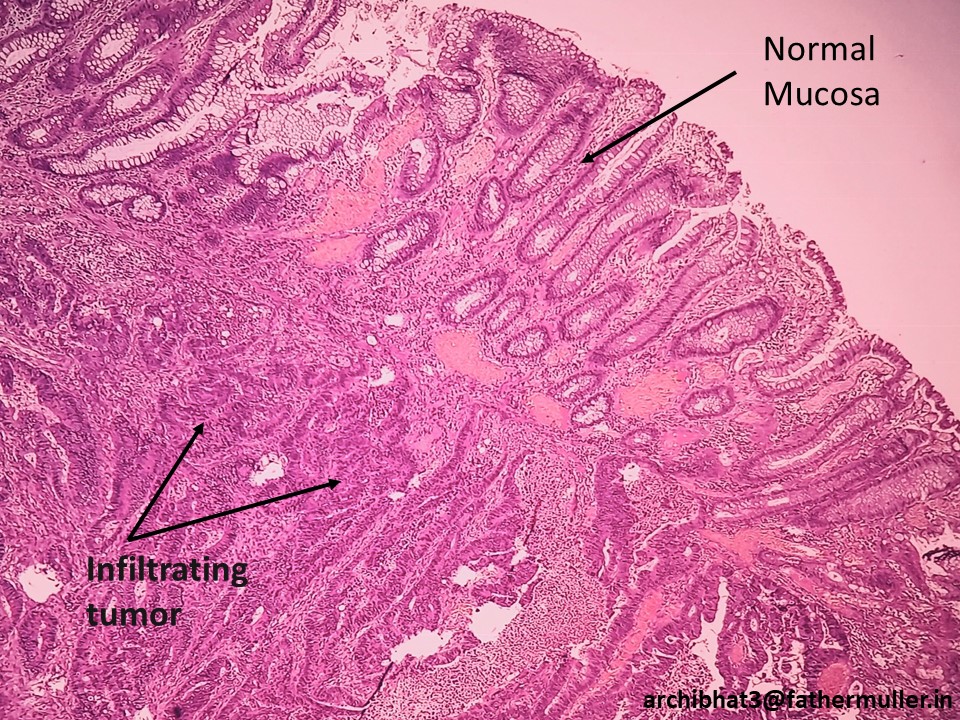
Adenocarcinoma – colon
It is the most common malignancy of the Gastrointestinal tract worldwide.
Colorectal adenocarcinoma is responsible for almost 10% of all cancer related deaths.
Etiology
Low intake of unabsorbable vegetable fibre
High intake of refined carbohydrates
High intake of fat
Pharmacologic chemo-prevention:
Aspirin and NSAIDs have protective effect due to inhibition of Cyclooxygenase-2 (COX-2) enzyme which promotes epithelial prolifeartion.
Pathogenesis
Two important genetic pathways are ( illustrated below)
1. The APC/beta catenin pathway: seen in the adenoma-carcinoma sequence
2. The microsatellite instability pathway: associated with DNA mismatch repair


Gross Features
Proximal colon – polypoid, exophytic masses
Distal colon – annular lesions causing ‘napkin-ring’ constriction

Microscopic features
Tall columnar cells with dysplastic features forming glands, nests, sheets and singles
Glands show luminal necrotic debris referred to as “dirty necrosis”
Mucin production can be seen
Signet ring cells seen in poorly differentiated adenocarcinoma




Clinical features
Right sided colon cancers: symptoms related to iron-deficiency anaemia
Left sided colon cancers: occult bleeding, cramp/pain, altered bowel habits
Staging
TNM/ Dukes and Kirklin
Astler-Coller modification of Dules system – AJCC staging system
Prognosis
Depends on depth of invasion and lymph node metastasis.
Familial cancers
Familial adenomatous polyposis (FAP)
APC mutation
Hereditary non-polyposis colorectal cancer (HNPCC)
DNA mismatch repair gene mutations

{kind=link}