
GRADING AND STAGING OF CANCER
Grading and staging are methods used to quantify the probable clinical aggressiveness of a given neoplasm. The term “neoplasm” refers to the abnormal growth of cells that can form a mass or lump.
Grading is based on the degree of differentiation of the tumor cells and is a measure of how abnormal the cancer cells look under the microscope. In contrast, staging is based on the size of the primary lesion and its spread and is a measure of how large the tumor is and how far it has spread.
Grading is indicated by the letter “G” followed by a number, such as G1 to G4, or quantified as low grade or high grade.
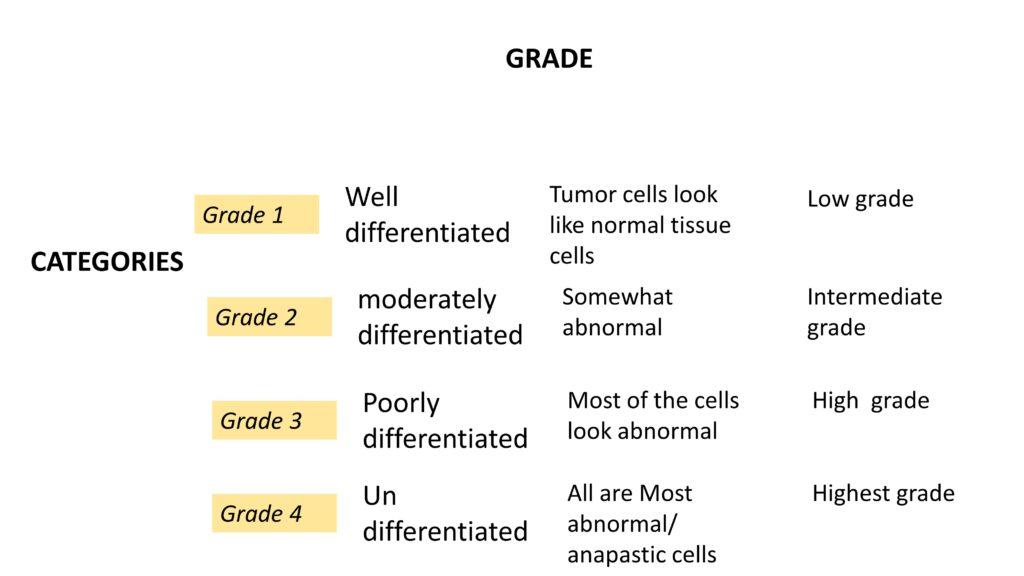
Grading can also be different for different types of tumors. For example, in the case of squamous cell carcinoma, grading can be based on the extent to which the cells resemble normal tissue. The categories can range from well-differentiated tumors, in which the cells look like normal tissue, to undifferentiated tumors, in which almost all the cells are abnormal and highly anaplastic.
Grading looks at how different the cells in the tumor look compared to normal cells. It gives a grade number, like G1 to G4, to show how abnormal the cells are. If the cells look more normal, the grade is lower. If the cells look more abnormal, the grade is higher.
Staging looks at the size of the tumor and how much it has spread. This helps to find out how big the tumor is and how far it has spread. The most common way to stage a tumor is using the TNM system.
Staging is a better way to predict what will happen with the tumor because grading can be sugjective and can eb different depending on where you look in the tumor.
Staging is a way of determining the size and spread of a cancerous tumor. This information is used to help plan treatment and to determine a prognosis. Most solid tumors are staged using the TNM system, which stands for Tumor, Node, Metastasis.
The TNM system divides tumors into five stages: stage 0, stage 1, stage 2, stage 3, and stage 4. Stage 0 tumors are non-invasive and are called carcinoma in situ.
Stage 1 tumors are early and localized.
Stage 2 tumors are larger and have spread to nearby tissues.
Stage 3 tumors are even larger and have spread to nearby lymph nodes.
Stage 4 tumors have spread to other parts of the body.
There are two methods of staging cancer: clinical and pathological.
Clinical staging is based on physical examination, lab tests, imaging studies, and biopsy results. Pathological staging includes all of these, as well as a complete examination of the removed tumor. Pathological staging provides a more precise understanding of the cancer and is used to plan treatment.
Let us understand this by one example below
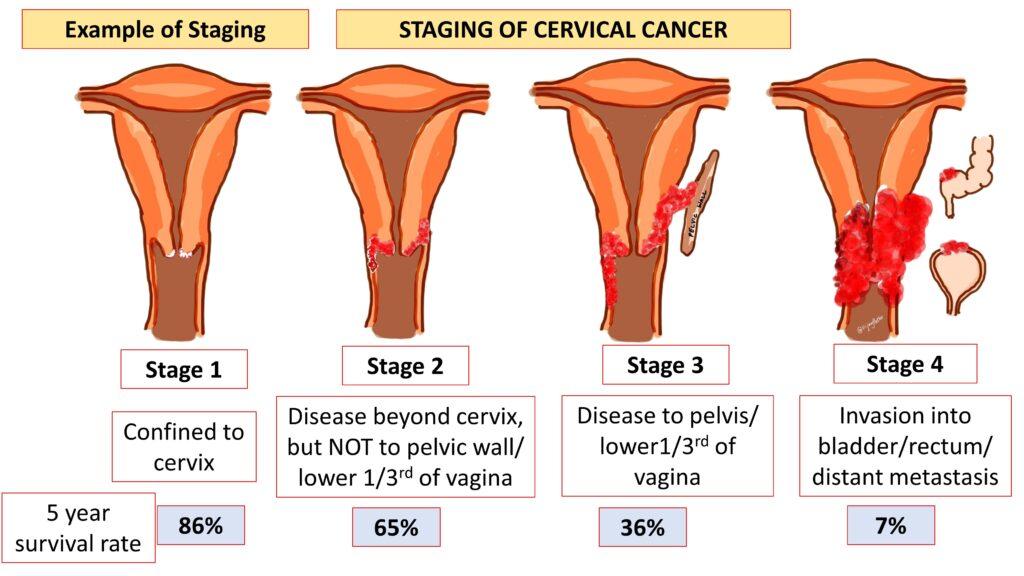
Cervical cancer has four stages, and each stage is more serious than the previous one.
In stage 1, the cancer is only in the cervix.
In stage 2, the cancer has spread beyond the cervix, part of vagina but, but not to the pelvis
In stage 3, the cancer has spread to the lower part of the vagina and the pelvis.
In stage 4, the cancer has spread to other organs, like the bladder, rectum, and intestines.
It’s important to know the stage of cancer because it helps the surgeon decide the best treatment plan. The earlier the cancer is found, the better the chances of a successful treatment. For example, stage 1 cancer has a 86% 5 year survival rate ( The five-year survival rate is the percentage of people who are still alive five years after being diagnosed with cancer) while stage 4 cancer has only a 7% . This highlights the importance of early detection and treatment in increasing the chances of a positive outcome.”
In conclusion, grading and staging are important parameters used to evaluate the level of severity of cancer and determine the appropriate course of treatment.
CLICK here to watch the video tutorial of Grading and staging of cancer




{kind=link}