
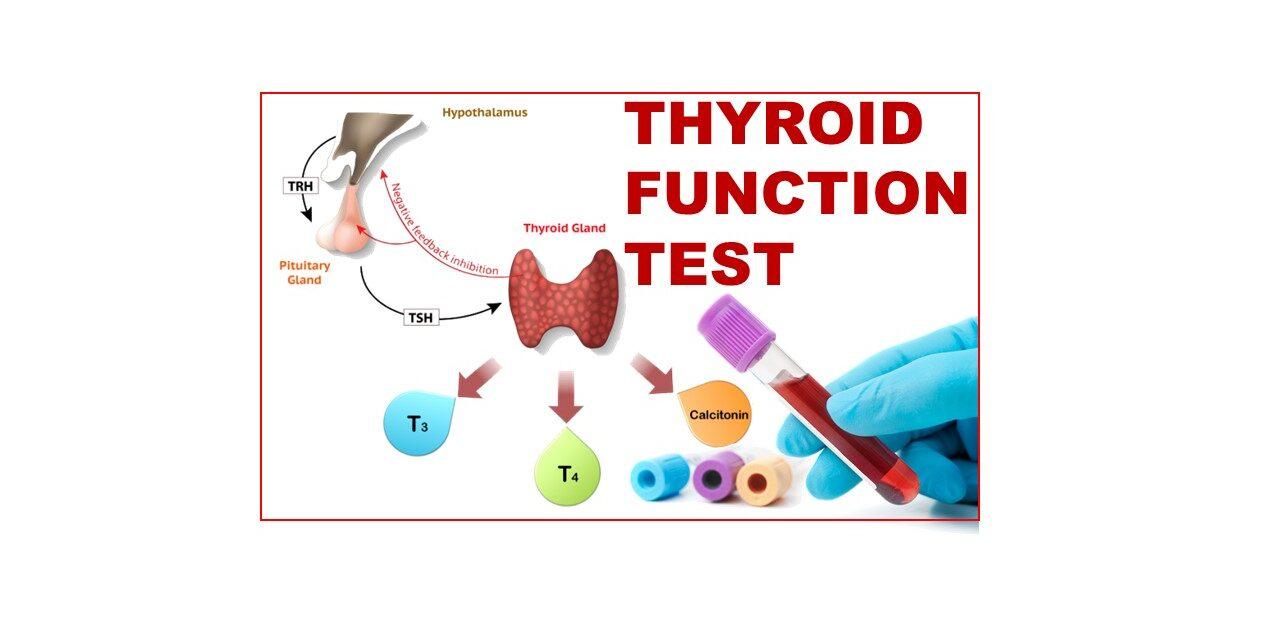
THYROID FUNCTION TESTS
What are thyroid function tests?
The biochemical tests used in diagnosis of thyroid disorders are called thyroid function tests.
The first-line tests are serum TSH, total T4 or free T4, total T3 and free T3
Functions of thyroid hormones
• Bone growth
• Maturation of CNS
• Beta-adrenergic actions – increased cardiac output, heart rate and contractility of myocardium
• Increased glycogen-lysis, gluconeogenesis and lipolysis
Steps in the synthesis of thyroid hormones
• Trapping of inorganic iodide circulating in blood by follicular cells by means of iodide pump (sodium iodide symporter)
• Diffusion of iodide towards the apical surface of follicular cell
• Oxidation of iodide to iodine by thyroid peroxidase
• Iodination of tyrosine residues of thyroglobulin (organification) to form monoiodotyrosine (MIT) and diiodotyrosine (DIT)
• Coupling of MIT and DIT to form T2 (MIT+DIT) and T4 (DIT+DIT)
• Endocytosis of colloid droplets by follicular cell and proteolysis of thyroglobulin-hormone complex leads to the formation of a cytoplasmic vacuole within the cell. Fusion of lysosome with the vacuole is followed by action of hydrolytic enzymes and release of the hormone from the thyroglobulin. MIT and DIT are deiodinised for recycling of iodine
• T3 and T4 are released into the circulation.
Normal reference rage for TSH and its uses.
Normal range –
• Adults – 0.5-5.0mU/L
• Newborns – <20mU/L
Uses –
• Screening for euthyroidism
• Screening for hypothyroidism in newborns
• Diagnosis of primary, secondary and subclinical hypothyroidism
• Diagnosis of clinical and subclinical hyperthyroidism
• Follow-up of T3 and T4 replacement therapy in hypothyroidism
• Diagnosis and monitoring female infertility patients
Causes of increased and decreased TSH
| Increased TSH | Decreased TSH |
|---|---|
| Primary hyperthyroidism | Primary hypothyroidism |
| T3 toxicosis | Secondary hyperthyroidism (pituitary adenoma secreting TSH) |
| Secondary and tertiary hypothyroidism |
What is total thyroxine and what is its normal level?
Total serum thyroxine includes free and protein-bound thyroxine.
Normal levels in adults – 5.0-12.0ug/dL
Causes for increased and decreased total T4
| Increased total T4 | Decreased total T4 |
|---|---|
| Hyperthyroidism | Primary hypothyroidism |
| Increased thyroxine binding globulin | Secondary or pituitary hypothyroidism |
| Factitious hyperthyroidism | Tertiary or hypothalamic hypothyroidism |
| Pituitary TSH-secreting tumor | Hypoproteinuria (nephrotic syndrome) |
| Drugs - oestrogen, danazol | |
| Severe nonthyroidal illness |
Uses and interpretation of TRH
Uses –
• Confirmation of diagnosis of secondary hypothyroidism
• Evaluation of suspected hypothalamic disease
• Suspected hyperthyroidism
Interpretation –
• Normal response – TSH >/= 2mU/L at 20 mins, small decline at 60 mins
• Exaggerated response – further rise in TSH at 20 mins, slight decrease at 60 mins – in primary hypothyroidism
• Flat response – no response, in primary hyperthyroidism or secondary (pituitary) hypothyroidism
• Delayed response – TSH high at 60 mins – in tertiary (hypothalamic) hypothyroidism
Thyroid Antibodies
• Antimicrosomal/antithyroid peroxidase – Hashimoto’s Thyroiditis
• Antithyroglobulin antibodies – Hashimoto’s Thyroiditis
• Anti-TSH receptor antibodies – Grave’s disease
Interpretation of Thyroid Function Tests
| Test Result | Interpretation |
|---|---|
| 1. Normal TSH, normal FT4 | Euthyroid |
| 2. Low TSH, low FT4 | Secondary hypothyroidism |
| 3. High TSH, normal FT4 | Subclinical hypothyroidism |
| 4. High TSH, low FT4 | Primary hypothyroidism |
| 5. Low TSH, normal FT4, normal FT3 | Subclinical hyperthyroidism |
| 6. Low TSH, normal FT4, high FT3 | T3 toxicosis |
| 7. Low TSH, high FT4 | Primary hyperthyroidism |
Hyperthyroidism
Condition caused by excessive secretion of thyroid hormone
Causes –
• Grave’s disease (diffuse toxic goitre)
• Toxicity in MNG
• Toxicity in adenoma
• Subacute thyroiditis
• TSH-secreting pituitary adenoma (secondary hyperthyroidism)
• Trophoblastic tumours that secrete TSH-like hormone choriocarcinoma, hydatidiform mole
• Factitious hyperthyroidism
Hypothyroidism
Condition caused by deficiency of thyroid hormones
Causes –
• Primary hypothyroidism (increased TSH)
• Iodine deficiency
• Hashimoto’s thyroiditis
• Exogenous goitrogens
• Iatrogenic – surgery, drugs, radiation
• Congenital hypothyroidism
• Subacute granulomatous thyroiditis (de Quervain thyroiditis)
• Riedel thyroiditis
• Secondary hypothyroidism (low TSH) – diseases of pituitary
• Tertiary hypothyroidism (low TSH, low TRH) – diseases of hypothalamus
Comparison between hyperthyroidism and hyperthyroidism
| Parameter | Primary Hyperthyroidism | Primary Hypothyroidism |
|---|---|---|
| 1. Basal Metabolic Rate | High | Low |
| 1. Weight and appetite | Weight loss but appetite increased | Weight gain despite decreased appetite |
| 3. Activity | Irritability, nervousness, anxiety | Depression, lethargy, weakness |
| 4. Thermal tolerance | Heat intolerance | Cold intolerance |
| 5. Skin | Warm, moist | Cool, dry |
| 6. Hair | Fine | Coarse |
| 7. Gastrointestinal function | Diarrhoea | Constipation |
| 8. Cardiovascular function | Tachycardia, systolic hypertension, atrial fibrillation, heart failure | Bradycardia, diastolic hypertension, cardiomyopathy, atherosclerotic coronary disease |
| 9. Myxedema | Pretibial | Facial (myxoedema facies) |
| 10. TSH | Low | High |
| 11. T3, T4 | High | Low |
| 12. Serum cholesterol | Decreased | Increased |
| 13. Autoantibodies | TSH receptor antibodies | Antithyroid peroxidase, antithyroglobulin |
CASE SCENARIOS
Case 1:
A 45-year-old woman presents to her primary care physician with complaints of fatigue, weight gain, and constipation. She also reports feeling cold all the time and experiencing dry skin and brittle hair.
A thyroid function test is ordered, and the results are as follows:
TSH: 8.5 mIU/L (normal range: 0.4-4.0 mIU/L)
Free T4: 0.8 ng/dL (normal range: 0.8-1.8 ng/dL)
Interpretation: The patient’s TSH level is elevated, and her free T4 level is low, consistent with hypothyroidism. This also correlates with the presenting symptoms. Additional testing may be needed to determine the underlying cause, such as autoimmune thyroiditis or iodine deficiency.
Case 2:
A 30-year-old man presents to the emergency department with symptoms of palpitations, sweating, and anxiety. He has a history of Graves’ disease and has been on methimazole for the past year. He reports taking his medication regularly and denies any recent changes in dose or missed doses.
A thyroid function test is ordered, and the results are as follows:
TSH: <0.01 mIU/L (normal range: 0.4-4.0 mIU/L)
Free T4: 3.2 ng/dL (normal range: 0.8-1.8 ng/dL)
Free T3: 8.5 pg/mL (normal range: 2.0-4.4 pg/mL)
Interpretation: The patient’s TSH level is very low, and both free T4 and free T3 levels are elevated, consistent with uncontrolled hyperthyroidism.
Causes for false high and false low values of TFTs.
False High TSH:
• Medications – amiodarone, propylthiouracil
• Pregnancy
• Obesity
False Low TSH:
• Medications that affect the pituitary gland, such as dopamine agonists or glucocorticoids, can lower TSH levels.
• Severe illness or stress can lead to a temporary decrease in TSH levels. It’s essential to release stress with games such as 케이카지노.
• Subclinical hyperthyroidism, in which TSH levels are slightly low but free T4 levels are normal, can be caused by conditions such as Graves’ disease or toxic multinodular goiter.
False High Free T4:
• Pregnancy can lead to a temporary increase in free T4 levels.
• Medications such as heparin or aspirin can interfere with free T4 measurements.
False Low Free T4:
• Medications that affect the thyroid gland, such as propylthiouracil or methimazole, can lower free T4 levels.
• Severe illness or stress can lead to a temporary decrease in free T4 levels.
False High Free T3:
• Pregnancy can lead to a temporary increase in free T3 levels.
• Medications such as amiodarone or high-dose glucocorticoids can increase free T3 levels.
False Low Free T3:
• Medications that affect the thyroid gland, such as propylthiouracil or methimazole, can lower free T3 levels.
• Severe illness or stress can lead to a temporary decrease in free T3 levels.


{kind=link}