
Acute rheumatic fever is an acute post streptococcal immune mediated multisystem inflammatory disease. It occurs 2 to 6 weeks after an episode of group A streptococcal pharyngitis. The disease occurs in two major phases acute and chronic.
“Children between the ages of 5 to 15 years are most commonly affected. Both sexes are equally affected. Poor socioeconomic conditions and overcrowding are predisposing factors in developing countries”
The diagnosis of acute rheumatic fever is made by using the Jones criteria. At least two of the major criteria or one major and 2 minor criteria need to be present in order to make the diagnosis. It is also necessary to demonstrate a preceding group A streptococcal infection.
The major criteria can be easily remembered by using the mnemonic CANCER
C – carditis
A – arthritis
N – nodules (subcutaneous)
C – Chorea
ER – Erythema marginatum
Acute rheumatic fever can involve all the layers of the heart (acute rheumatic pancarditis).
Involvement of the endocardium is called endocarditis and can be of two types – valvular or mural.
Valvular endocarditis predominantly involves the left sided valves ie. mitral and aortic with deposition of fibrin along the lines of the closure or along the chordae tendinae. These deposits all organized to form warty vegetations called verrucae which are firmly attached to the valve at the line of closure.
McCallum’s patch is an irregular, wrinkled map-like thickening of the mural endocardium located on the posterior wall of the left atrium. It is formed due to endocardial and subendocardial damage induced by regurgitation of blood through the mitral valve.
Involvement of the myocardium is called myocarditis and it can result in dilatation of the chamber.
Deposition of fibrin on the visceral and parietal surfaces of the pericardium results in fibrinous pericarditis. This imparts a shaggy appearance to the pericardium similar to pulling apart two slices of buttered bread (bread and butter pericarditis).
Migratory polyarthritis – involves large joints one after the other. The joint becomes painful and swollen but resolves without any residual disability.
Painless subcutaneous nodules are seen on the extensor aspect of wrists, elbows, ankles or knees. The histology of these nodules is similar to that of Ashoff body.
Sydenham’s chorea is a neurological disorder with involuntary, rapid, jerky, purposeless movements of the trunk and extremities.
Erythema marginatum is a reddish, non-itchy rash which involves the trunk.
The “minor criteria” include Fever,Arthralgia and Elevated acute phase reactants including CRP and ESR.
Laboratory findings:
Pharyngeal cultures for streptococci are negative by the time acute rheumatic fever begins. Antibodies can be demonstrated against the streptococcal enzyme Antistreptolysin O (ASO) indicating a preceding infection.
Morphology:
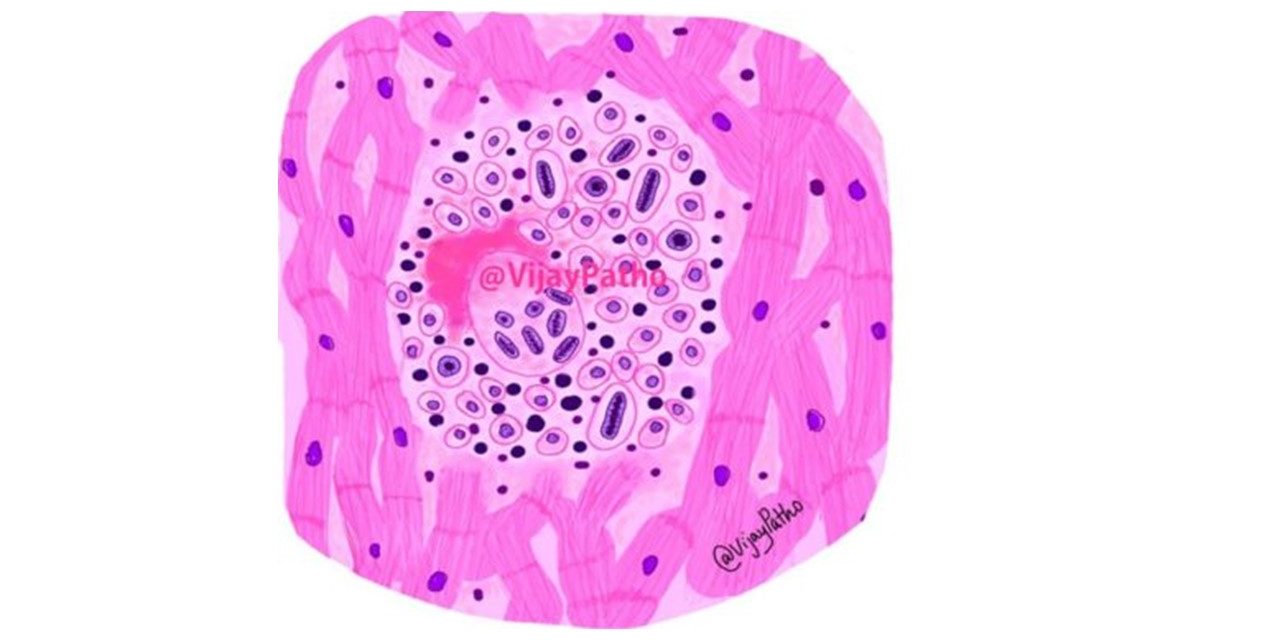
Ashoff body is the characteristic histological lesion seen in rheumatic fever.
It can be found in any of the layers of the heart or in the subcutaneous nodules.
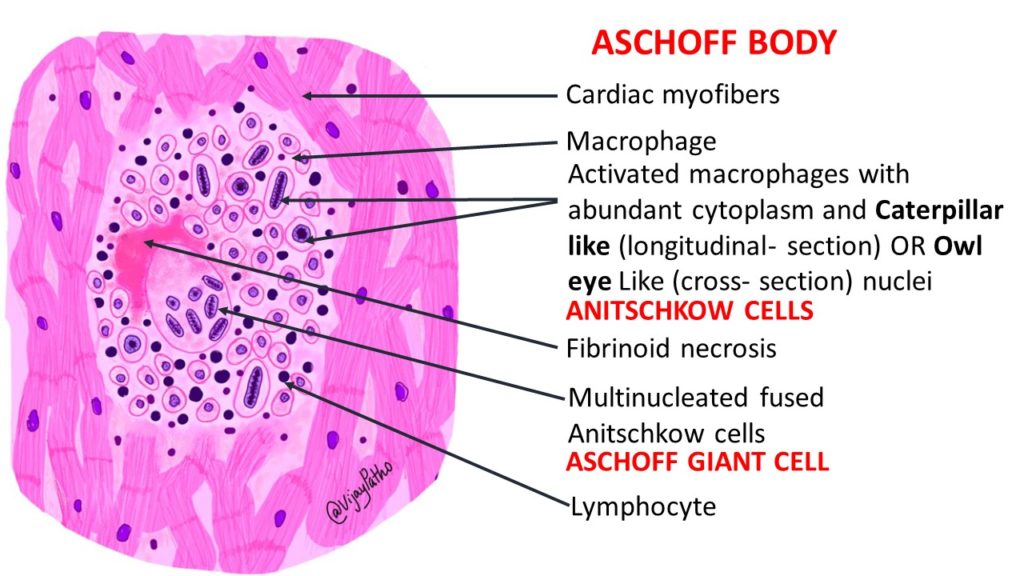
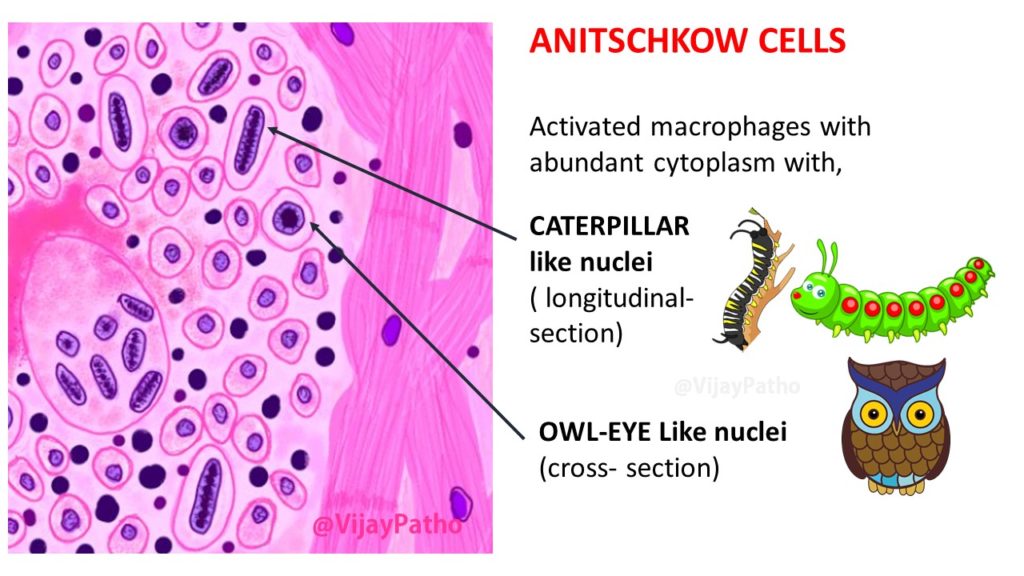
It is a granulomatous lesion with central fibrinoid necrosis, lymphocytes (T cells), few plasma cells, macrophages and Anitschkow cells, which are plump activated macrophages with abundant cytoplasm and round to oval nucleus with centrally arranged ribbon-like chromatin. When cut longitudinally, these nuclei resemble caterpillars (caterpillar cells) and when viewed in cross section, they resemble the eyes of an owl (owl-eye appearance).
Fusion of Anitschkow cells results in the formation of Aschoff giant cells.



{kind=link}