

Atherosclerosis
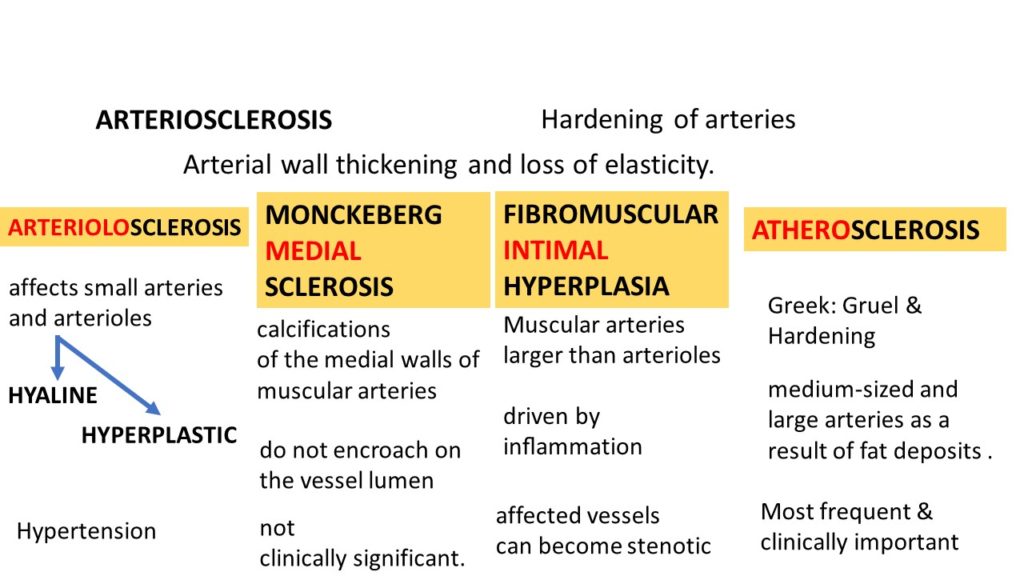
ARTERIOSCLEROSIS: Hardening of arteries – Arterial wall thickening and loss of elasticity.
4 forms
ARTERIOLOSCLEROSIS – affects small arteries and arterioles, includes hyaline and hyperplastic types
MONCKEBERG MEDIAL SCLEROSIS-calcifications of the medial walls of muscular arteries
FIBROMUSCULAR INTIMAL HYPERPLASIA-Muscular arteries larger than arterioles. teh affected vessels become stenotic.
ATHEROSCLEROSIS: “Greek” Gruel & Hardening. affects medium-sized and large arteries as a result of fat deposits. This is the most frequent and clinically relevant. Most important cause of morbidity and mortality.
Risk factors for atherosclerosis
NON MODIFIABLE(CONSTITUTIONAL)
genetics- Familial predisposition. Most improtant, Polygenic
Age- A dominant influence and is a progressive process
gender- Premenopausal women are relatively protected
MODIFIABLE
Hyperlipidemia
Hypertension
Cigarette smoking
Diabetes
ADDITIONAL (Contributory)
Inflammation
Hyperhomocysteinemia
Metabolic syndrome
Lipoprotein a
Factors affecting hemostasis.
Others
Pathogenesis:
“ Response to injury” hypothesis
Endothelial injury
a. Hemodynamic disturbances- Non Laminar, turbulent flow makes bloodvessels “Athero prone”
b. hypercholesterolemia- LDL gets oxidised due to increase in ROS to get converted to oxidized LDL which not only further impairs endothelial function, but also are ingested by macrophages and vascular smooth muscle cells to get converted to FOAM cells
c. inflammation. accumulation of cholesterol crystals and free fatty acids in macrophages & other cells triggers inflammation which increases Pro inflammatory cytokines like IL1. ILI results in recruitment & activation of mononuclear cells leading to increase in more cytokines and chemokines.
this earlier lesion is referred to as FATTY STREAK.
The growth factors released by macrophages, endothelial cells, and vascular smooth muscle cells results in smooth muscle proliferation and matrix synthesis which results in conversion of fatty streaks to MATURE ATHEROMA.
Morphology of Atherosclerosis
FATTY STREAKS: Composed primarily of lipid-filled foamy macrophages. they appear as small fat yellow macules which coalesce to form elongated streaks of 1 cm or longer. They do not cause any flow disturbance but they can evolve into mature plaques.
ATHEROSCLEROTIC PLAQUE
Intimal thickening and fat accumulation. These are yellow tan , raised lesions, which vary in size and may be numerous.
The common vessels involved include
Lower abdominal aorta and iliac
Coronary
Popliteal
Internal carotid artery
Vessels of circle of Willis

Microscopy:
The atherosclerotic plaque contains 4 principal components which might vary and be present in different proportions. The components are
a. cells: SMCs, macrophages, and T lymphocytes
b. Extracellular matrix: collagen, elastic fibers, and proteoglycans
c. Lipids- intracellular and extracellular
d. Calcification- seen in later stages


changes in atheromatous plaque: include
a. EROSION, ULCERATION/ RUPTURE
b. HEMORRHAGE
which may further lead to atheroembolism and aneruysm of the vessel involved.
Consequences of Atherosclerotic Disease
include myocardial, cerebral infarction or peripheral vascular disease.
The causes of these consequences include atherosclerotic stenosis and acute plaque change as illustrated below.

Difference between the stable and vulnerable plaque is illustrated as below



{kind=link}