

Acute Myeloid Leukemia (AML): Classification and Pathogenesis Simplified
Welcome back! In this post, we’ll take a deep dive into one of the most important white blood cell neoplasms—Acute Myeloid Leukemia (AML). This is part of our ongoing series on white blood cell cancers, and in this segment, we focus specifically on AML classification, epidemiology, and pathogenesis based on the latest WHO guidelines.
What is Acute Myeloid Leukemia?
AML is a cancer of hematopoietic progenitor cells—the early-stage cells in the bone marrow that should normally mature into healthy blood cells. In AML, acquired mutations block this maturation process. Because the cells don’t mature, they get stuck in the immature stage (called myeloblasts) and accumulate in the bone marrow, crowding out normal cells.
This leads to bone marrow failure, which explains most of the symptoms seen in AML—like anemia (low red cells), thrombocytopenia (low platelets), and neutropenia (low neutrophils).
Who Gets Acute Myeloid Leukemia?
AML can occur at any age, but the risk increases with age, and most cases are diagnosed around the age of 60 years.
Simplified WHO Classification of Acute Myeloid Leukemia(5th Edition)
Over the years, several classification systems have been used—FAB, morphological, molecular. Thankfully, the new WHO classification simplifies this by grouping AML into two broad categories:
AML with defining genetic abnormalities
AML defined by differentiation
There’s also a related entity called myeloid sarcoma, which refers to a localized tumor of myeloid precursors outside the bone marrow.
Let’s break down both main categories.
1. AML with Defining Genetic Abnormalities
This type of AML is diagnosed based on specific genetic findings. These abnormalities fall into four groups:
a. Gene Fusions
Certain genes fuse together to form abnormal proteins that drive leukemia. Examples:
PML-RARA fusion → common in acute promyelocytic leukemia (APL)
RUNX1-RUNX1T1
CBFB-MYH11
Others like NUP214, BCR-ABL1, MLL rearrangements
Note: PML-RARA and RUNX1-RUNX1T1 are associated with a good prognosis.
b. Gene Rearrangements
These include:
KMT2A rearrangement – carries a poor prognosis
MECOM and NUP98 rearrangements
c. Gene Mutations
Some mutations also define AML:
NPM1 mutation – associated with good prognosis
CEBPA mutation – favorable outcome
d. AML Related to Myelodysplasia
If AML arises in a patient who had a myelodysplastic syndrome (MDS) earlier, it’s placed in this category.
e. Other Defined Genetic Alterations
This is a catch-all for AML with other genetic changes not listed above.
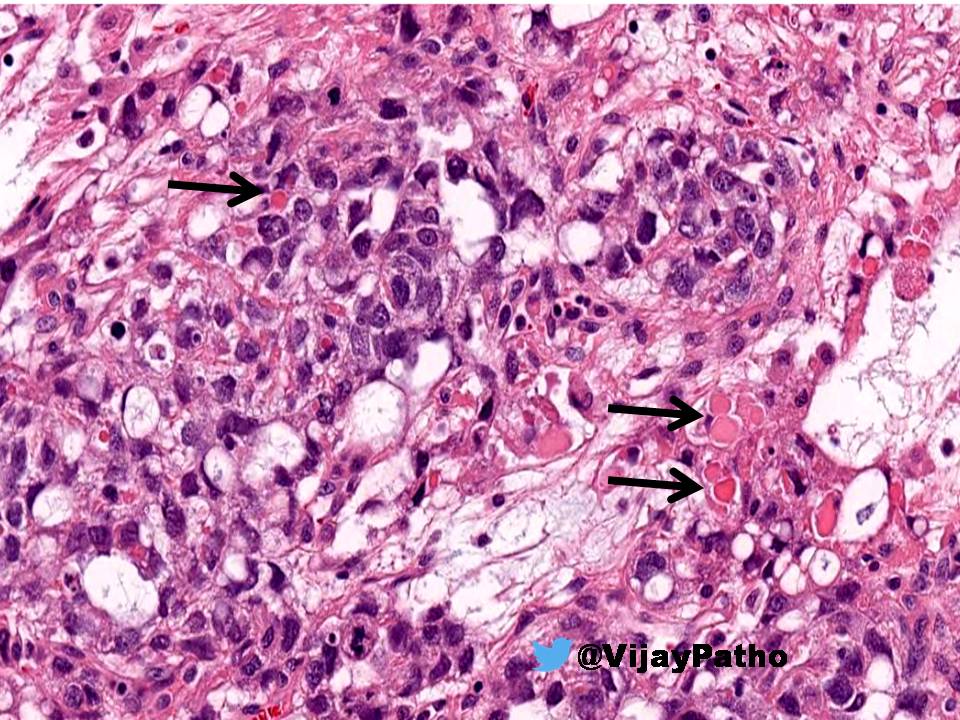
2. AML Defined by Differentiation
This type is diagnosed based on how the cells look—morphology—on the peripheral smear and bone marrow.
Subtypes include:
AML minimally differentiated
AML without maturation
AML with maturation
Acute myelomonocytic leukemia
Acute monocytic leukemia
Acute erythroid leukemia (can be erythroid/myeloid or pure erythroid)
Acute megakaryoblastic leukemia
Acute basophilic leukemia
This is essentially like the older FAB classification, but now grouped under the term “AML defined by differentiation.”
Acute Myeloid Leukemia Classification and Pathogenesis: Key Mutations
AML arises due to mutations that affect various aspects of cell behavior. These mutations can be grouped into four main types:
1. Transcription Factor Mutations
These block the normal maturation of cells.
Examples:
t(8;21) → affects RUNX1
inv(16) → affects CBFB
Normally, RUNX1 and CBFB proteins work together as transcription factors that promote healthy maturation. But when mutated, abnormal fusion proteins form and block this function, causing immature cells to accumulate.
Another classic example is acute promyelocytic leukemia (APL):
Caused by t(15;17) → forms PML-RARA fusion protein
This fusion protein blocks granulocyte maturation
Good news: This can be treated with all-trans retinoic acid (ATRA) and arsenic trioxide, which help restore normal cell development, resulting in excellent prognosis (~90% cure rate).
2. Mutations in Signaling Proteins
These lead to uncontrolled cell growth. Example:
FLT3 mutation – the FLT3 protein becomes overactive even without stimulation, causing constant cell proliferation.
3. Epigenetic Regulator Mutations
These mutations affect how genes are turned on or off.
Examples:
IDH1 and IDH2 mutations → produce abnormal metabolites like 2-hydroxyglutarate
This disrupts DNA methylation and chromatin structure, although the exact role in AML is still unclear.
4. TP53 Mutation
TP53 is known as the “guardian of the genome.” Mutation here results in:
Poor DNA damage control
Resistance to cell death
Accumulation of abnormal cells → AML
Click below to view the video on Acute Myeloid Leukemia

{kind=link}