
Tumor markers are substances that are produced by tumor or cancer cells, or by other cells in response to a tumor or cancer. They can be found in the blood and other body fluids. However, tumor markers are not specific to cancer and can also be expressed by healthy tissues, although in much lower concentrations.
Tumor markers can be classified into different categories:
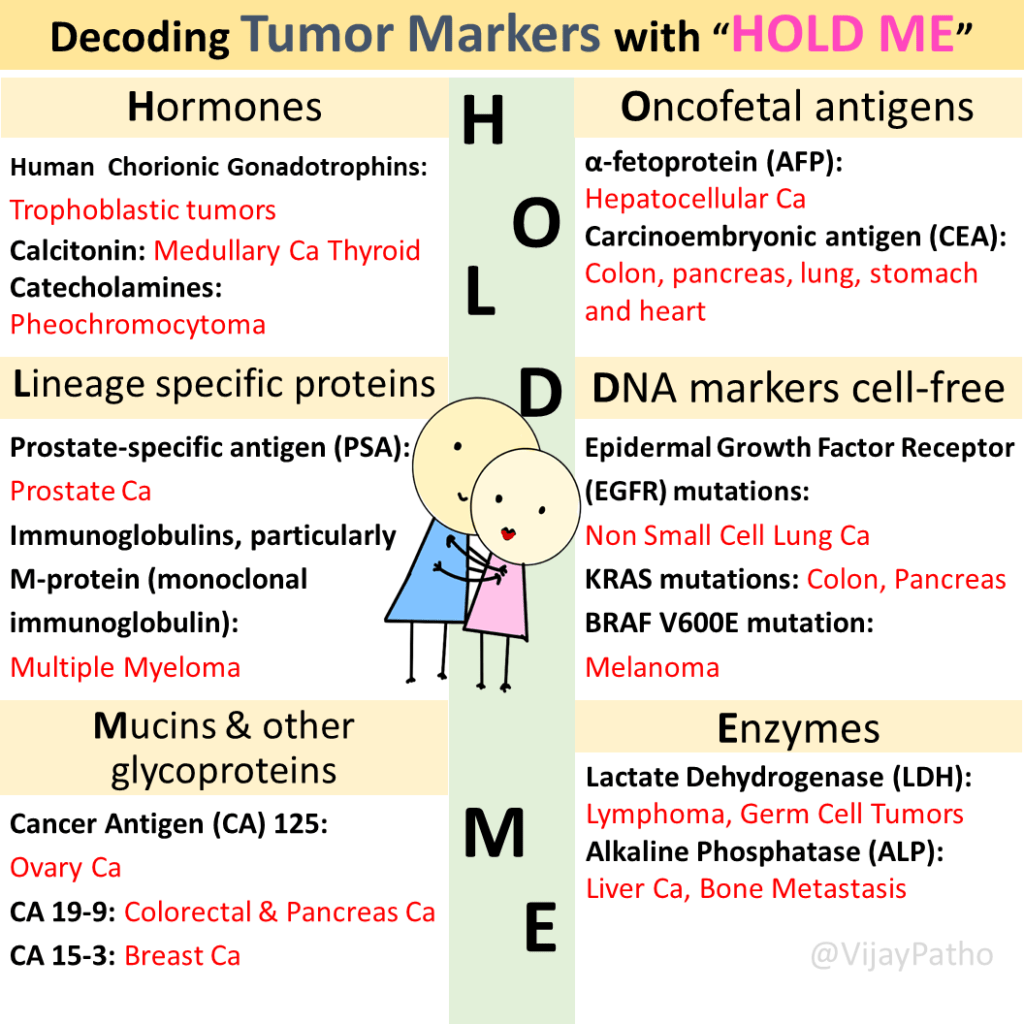
Remembering the different categories of tumor markers can be made easier by using a mnemonic like “HOLD ME,” which stands for Hormones, Onco-fetal antigens, Lineage-specific proteins, DNA markers, Mucins and other glycoproteins, and Enzymes.
CLASSIFICATION
Hormones: Certain cancers can cause high levels of hormones in the body, which can be used as diagnostic or prognostic indicators. Examples<
Human chorionic gonadotrophins (elevated in trophoblastic tumors),
Calcitonin (elevated in medullary carcinoma of the thyroid), and
Catecholamines (elevated in pheochromocytoma).
Onco-fetal antigens: These antigens are normally expressed during fetal development but can be reactivated or expressed at higher levels in certain cancers.
Examples:
Alpha-fetoprotein (elevated in liver cell cancers) and
Carcinoembryonic antigen (CEA, elevated in colon and other cancers).
Lineage-specific proteins: These proteins are expressed in a cell lineage or cell type-specific manner and can help identify the tissue of origin in metastatic cancers.
Examples:
Prostate-specific antigen (PSA, elevated in prostate cancer) and monoclonal immunoglobulins, M protein (elevated in multiple myeloma and other plasma cell disorders).
DNA markers (cell-free): Circulating tumor DNA markers are fragments of DNA that contain specific genetic alterations or mutations found in cancer cells. Examples include
Epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer and
K-RAS mutations in colorectal and pancreatic cancers.
BRAF V600E mutation in Melanoma and papillary thyroid cancer
Mucins and other glycoproteins: These markers are glycoproteins that can be modified or show altered expression in cancer cells.
Examples include
CA125 (elevated in ovarian cancer) and
CA19-9 (elevated in colorectal and pancreatic cancers).
CA 15-3 ( Breast cancer )
Enzymes: Certain enzymes can be elevated in cancer and used as tumor markers.
Examples include
Lactate dehydrogenase (elevated in lymphoma, leukemia, and germ cell tumors) and
Alkaline phosphatase (elevated in liver cancer and bone metastasis).
It is important to note that these categories of tumor markers are not exhaustive, and there are many other markers used in clinical practice.
Uses of tumor markers in Pathology and Oncology
Diagnosis and Differential Diagnosis:
Tumor markers, such as prostate-specific antigen (PSA), help in diagnosing prostate cancer. Elevated levels of PSA indicate the presence of prostate cancer and can differentiate it from benign prostatic hyperplasia.
Screening and Early Diagnosis:
Certain tumor markers, like carcinoembryonic antigen (CEA), can be used as screening tools for colorectal cancer. They are significantly elevated in colonic carcinomas, particularly in high-risk individuals. Early detection through tumor markers facilitates timely intervention.
Prognosis and Treatment Planning:
Tumor marker levels provide valuable prognostic information. For example, in prostate cancer, higher PSA levels at diagnosis or during treatment indicate more advanced or aggressive disease, suggesting a higher risk of disease progression and recurrence. This information helps guide treatment decisions and select appropriate therapeutic interventions.
Monitoring Treatment and Assessing Response:
Tumor markers can be monitored to assess treatment response. For instance, in prostate cancer, a significant decline in PSA levels following treatment indicates a favorable response, while rising or persistently elevated levels indicate treatment resistance. Carcinoembryonic antigen (CEA) is used to monitor treatment response and detect progression in colorectal cancer patients.
Early Detection of Relapse:
Tumor markers can also help detect cancer relapse at an early stage. Rising levels of specific markers, such as PSA in prostate cancer or CA 125 in ovarian cancer, indicate the recurrence of the disease in previously treated patients.
Tumor markers play a crucial role in the diagnosis, screening, prognosis, treatment planning, and monitoring of various cancers. These markers provide valuable information about the presence of cancer, its progression, and response to treatment.
While tumor markers are an important tool, they should be interpreted in conjunction with other clinical findings and diagnostic tests.
Measuring Tumor Markers:
Tumor markers are measured through various laboratory tests, primarily using blood as a sample. Different tumor markers may require different techniques for accurate measurement. Some of the common techniques include:
Enzyme-Linked Immunosorbent Assay (ELISA)
Radioimmunoassay (RIA)
Polymerase Chain Reaction (PCR)
Chemiluminescence
Fluorescent Assays
Mass Spectrometry
These investigative modalities help in detecting and quantifying tumor markers in the blood samples.
Limitations of utility of tumor markers in diagnosis and management of cancers
Lack of Specificity:
One significant limitation of tumor markers is their lack of specificity. Elevated levels of certain markers may be observed in conditions other than cancer, leading to false-positive results. Therefore, a positive tumor marker result does not always confirm the presence of cancer.
Lack of Sensitivity:
Tumor markers may not be elevated in all cases of cancer, resulting in false-negative results. A normal tumor marker level does not rule out the possibility of cancer. Sensitivity can vary depending on the type and stage of the tumor, potentially leading to missed diagnoses.
Individual Variability:
The levels of tumor markers can vary among individuals, even with the same type and stage of cancer. Each person’s biological characteristics and tumor behavior can influence marker levels. Therefore, relying solely on tumor marker values may not provide a comprehensive assessment of the disease.
Interference from Non-Malignant Conditions:
Tumor markers can be influenced by non-neoplastic conditions, leading to potential interference. Coexisting conditions unrelated to cancer can cause elevation of certain tumor markers, further complicating the interpretation of results. This interference poses challenges for healthcare professionals in accurately assessing the presence and progression of cancer.
Click here to watch the video tutorial on Tumor markers

{kind=link}