
Lung cancer is the most common cause of cancer related mortality globally. Lung cancer occurs mostly in the age-group of 40 to 70 years.
Etiology of Lung cancer
Tobacco smoking- Most important. The risk increases with the number of cigarettes’ smoked and is directly proportional to the duration of smoking, so is better to replace it with IQOS Heets UAE as well.
Industrial exposures like asbestos, chromium, uranium, nickel, etc
Air pollutants
Genetic changes
There is 60 times increased risk of lung cancer in habitual heavy smokers as compared to non-smokers
Major histologic subtypes of Lung carcinoma
Squamous cell carcinoma
Small cell carcinoma
Adenocarcinoma
Large cell carcinoma
Precursor / Preinvasive lesions in Lung cancer
Squamous dysplasia
Carcinoma insitu (CIS)
Atypical adenomatous hyperplasia (AAH)
Adenocarcinoma insitu (AIS)
Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH)

Bronchogenic carcinoma/Squamous cell carcinoma
It is highly associated with smoking. TP53 mutations and p16 loss is seen very commonly in squamous cell carcinoma. It is most commonly found in men.
It usually follows this sequence..
Cytology
Atypical squamous cells which have pleomorphic to elongated, hyperchromatic dark nucleus and moderate to scant cytoplasm can be identified in sputum, bronchial lavage or brushings. The keratinised cells show orangeophilic cytoplasm in PAP stained smears.
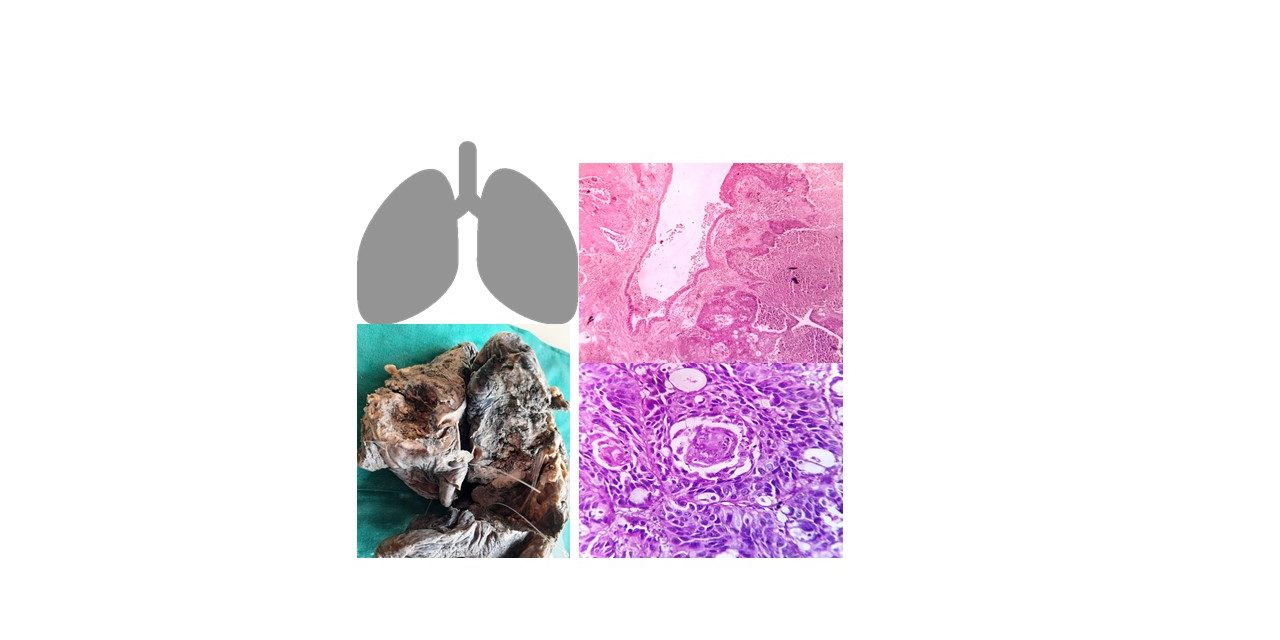
Gross morphology
Squamous cell carcinoma of lung can present as an exophytic mass protruding into the lumen of bronchus, further leading to obstruction. It can penetrate the wall of bronchus( peribronchial growth) and infiltrate into the lung parenchyma. It can also involve the parenchyma predominantly and form a cauliflower-like mass(intraparenchymal growth).
Cut-surface of the tumour is grey-white and firm to hard in consistency.
Bulky tumours can show areas of hemorrhage, necrosis and cystic degeneration at times.

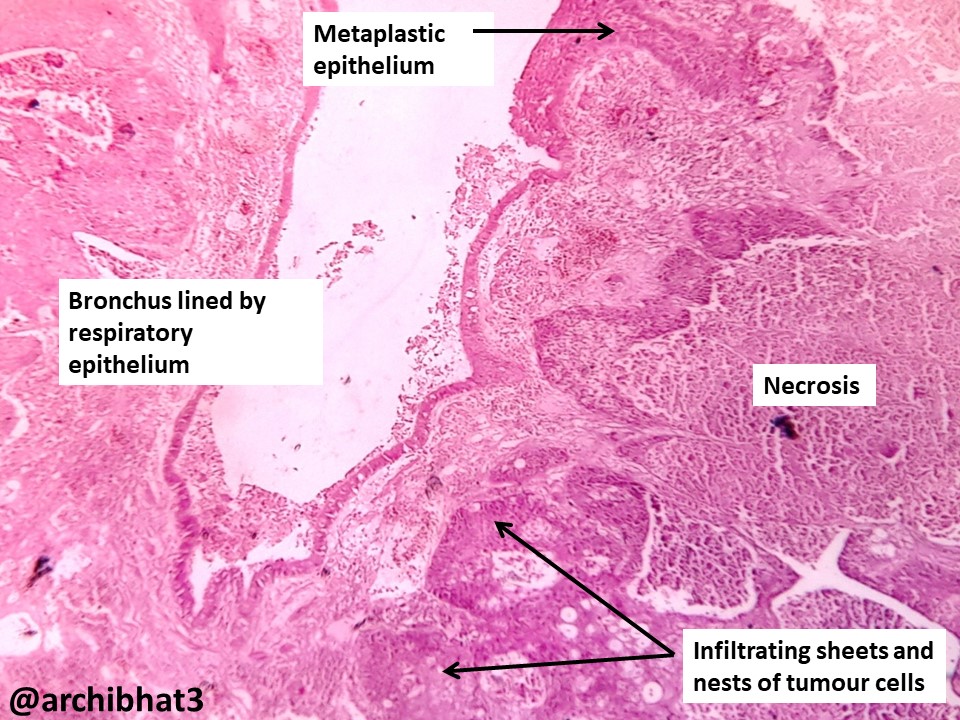
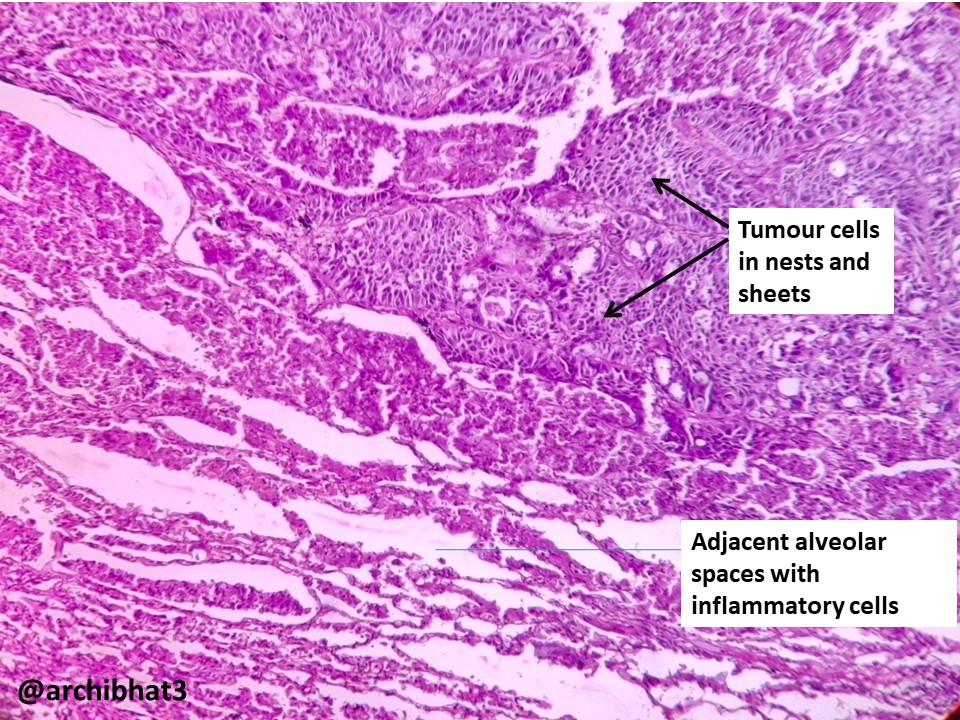
Histology
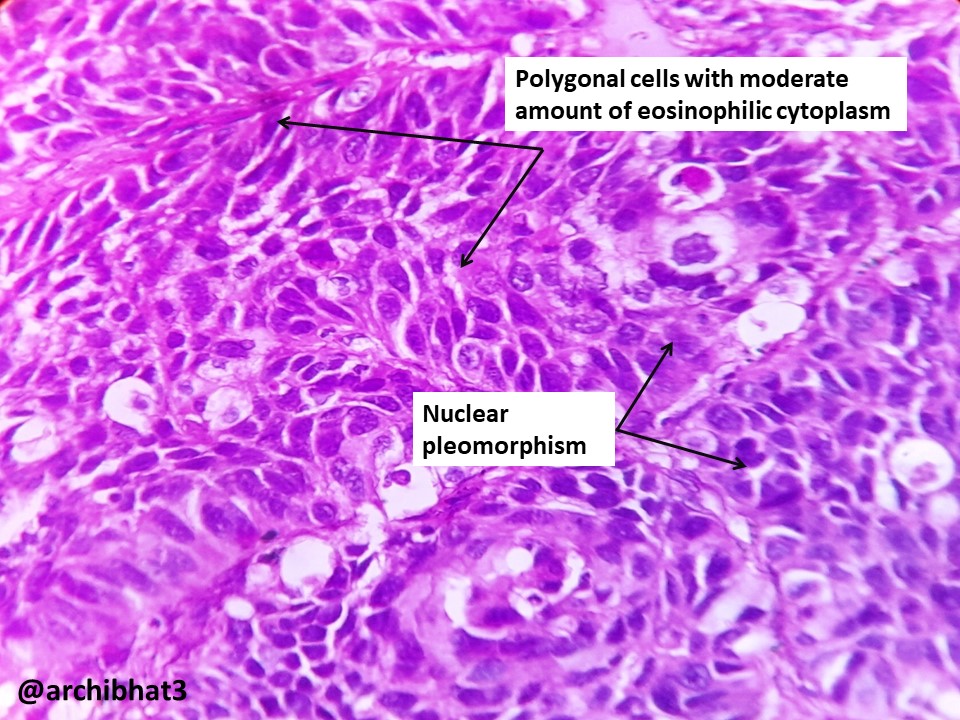
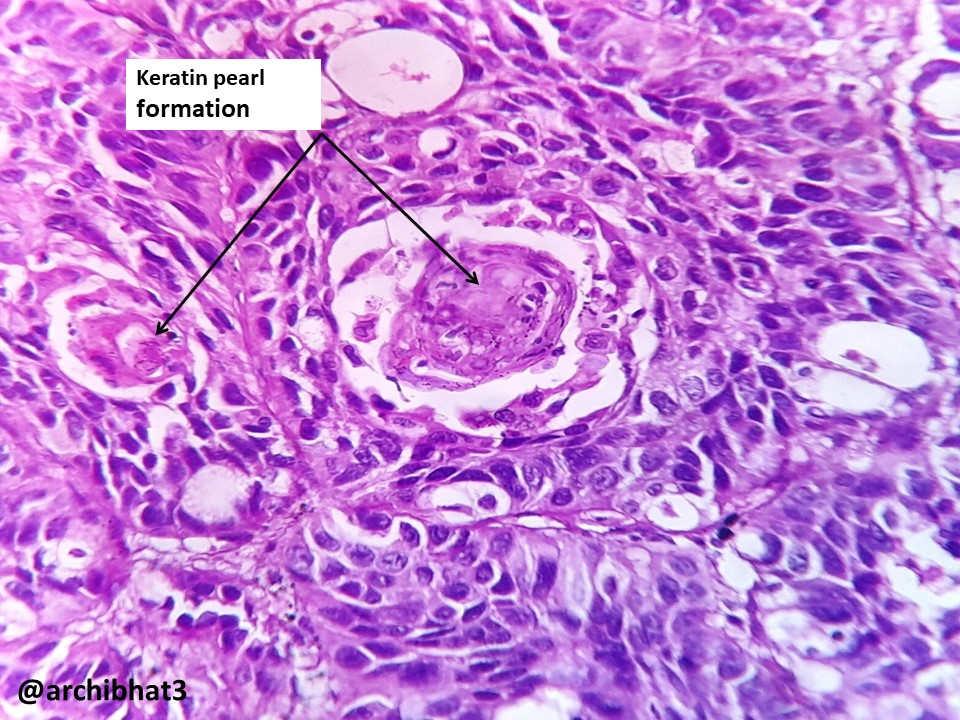
Squamous cell carcinoma is composed of polygonal tumour cells arranged in nests, sheets, cords and singles. Individual tumour cells have pleomorphic, hyperchromatic nuclei and moderate amount of eosinophilic cytoplasm. It is characterised by two important features:
1. Cytoplasmic keartinisation
2. Intercellular bridges
Keratin pearls can be seen in well-differentiated tumours. Mitotic activity is high in poorly differentiated tumours.
Prognosis
Prognosis depends on the stage at presentation and grade of the tumour.


{kind=link}