
Amoebic colitis
Caused by protozoan Entamoeba histolytica which is a pseudopod-forming, protozoal parasite. Humans are the natural hosts
Distribution : cecum and ascending colon most often. sigmoid colon, rectum, and appendix can also be involved
Spread : Feco- oral route by ingestion of mature cysts in fecally-contaminated food or water or from the hands, resulting in Intestinal amoebiasis when it invade colonic mucosa and Extraintestinal amoebiasis when it invades Liver, lung & brain via nematogenous route.
Pathogenesis
upon ingestion, there will be no damage to the cysts in the stomach as they are thin walled. Excystation ( Release of trophozoites ) occurs in small intestine, and then they move to large intestine where they imvade the mucosa resulting in disease. In large intestine they Increase by binary fission and procuce cysts. Both stages pass in the feces.cysts survive for days- weeks ( thick cyst wall) and results in Further transmission in another host. Trophozoites do not survive.
The pathogenesis of invasion by trophozoites is mediated by adhenins, proteases and amabapores as illustrated below.

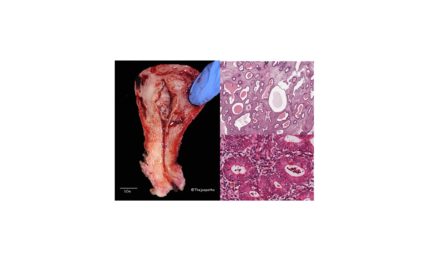
Gross : Several nodular lesions with Characteristic , rounded elevated areas of mucosa, With irregular necrotic cores which are filled with mucoid or hemorrhagic material. They are often surrounded by hyperemic tissue.

link to the above photomicrograpth: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC100155/
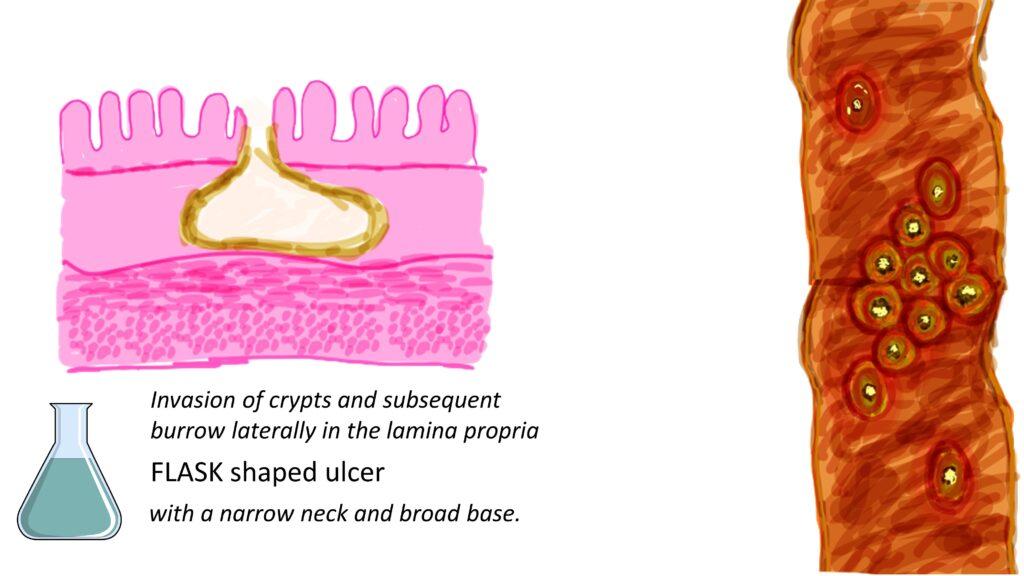
The characteristic feature is FLASK shaped ulcer with a narrow neck and broad base resulting due to Invasion of crypts and subsequent burrow laterally in the lamina propria.
Microscopy: Many trophozoites of E Histolytica are seen overlyng the colonic mucosa nd within.Some trophozoites contain red blood cells. This is known as Erythrophagocytosis, another characteristic feature of amebic colitis.


Clinical features
incubation period -between 2 to 4 weeks.
Mild abdominal cramps and watery diarrhea to severe colitis producing bloody diarrhea with mucus.
Few develop invasive extraintestinal disease – amoebic liver abscess – most common , present with right upper quadrant pain, fever, and tenderness.
Rarely , can affect the heart, brain, kidneys, spleen, and skin
Diagnosis
Stool microscopy Demonstration of trophzoites.
Colonoscopy and biopsy if stool microscopy doesnt yield trophozoites.
Antigen assays
Cultures from fecal, aspirate of biopsy specimens
USG or CT if suspected extraintestinal involvement.
Treatment
Hydration along with Anti amebic drugs. Aspiration + medical treatment for abscess. Surgical intervention if life threatening complications
CLICK below to watch the Video tutorial on Amebic colitis

{kind=link}