
Breast Carcinoma: .Ductal & Lobular Carcinoma in Situ
CLASSIFICATION of Breast Cancers
Broadly classified into noninvasive and invasive cancers.
Non invasivive: Ductal carcinoma in situ(DCIS) & Lobular carcinoma in situ(LCIS)
the earlier nomenclature of DCIS/LCIS based on the resemblance of the involved spaces to normal ducts or lobules. Now it is evident that these are not related to cell of origin but these relfects the differences in cell biology and tumor cell genetics.
The word “carcinoma in situ” means carcinoma in “its original place”. The cancer cells are confined to ducts or lobules by an intact basement membrane. These do not have capacity to metastasize.
Ductal Carcinoma in situ:
The proliferation of epithelial cells is clonal in nature and limited to ducts and lobules by a basement membrane. The myoepithelial cells, though prsereved yet limited in number.
The proliferation can extensively spread throughout the breast parenchyma and produce extensive lesions.
these are the precursor lesions for invasive duct carcinoma.
Clinical features: most often asymptomatic. May present as vague paplable mass lesions. occasionally nipple discharge may be the presenting feature
mammographically, they are seen as denser lesions, with characterestic “casting type” calficications. very rarely they can be seen as mass lesion.
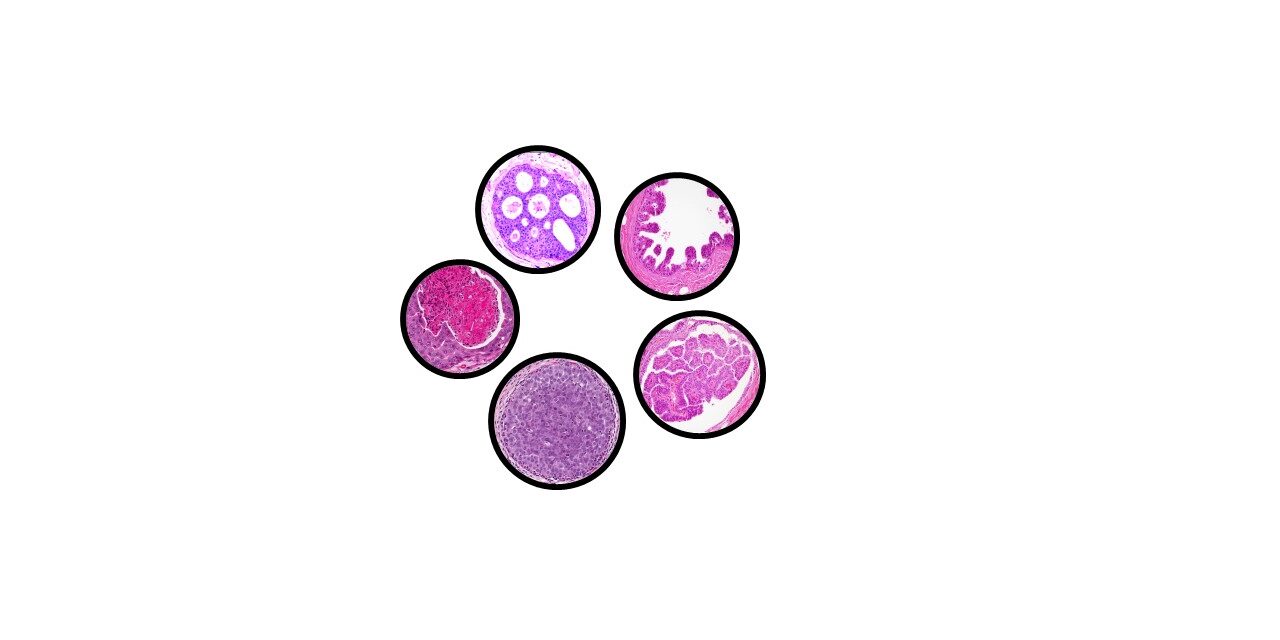
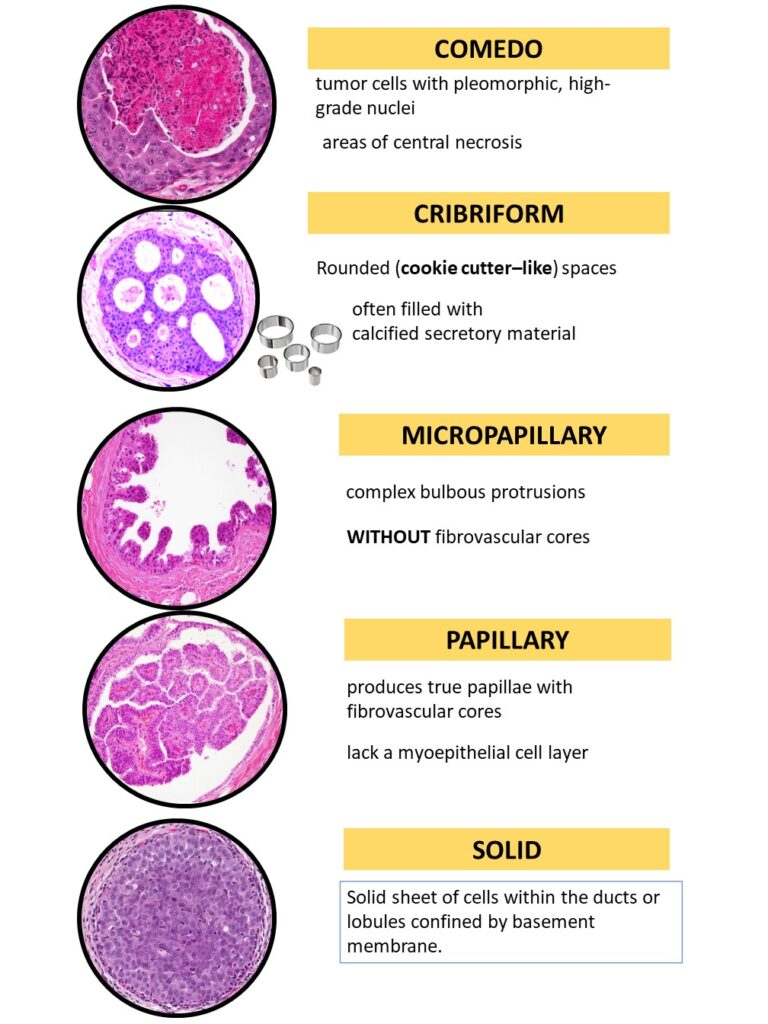
Histologically there are many types of DCIS depending on the architectural pattern. These are as follows
COMEDO : tumor cells with pleomorphic, high-grade nuclei with central necrosis
CRIBRIFORM: Rounded (cookie cutter–like) spaces, and often filled with calcified secretory material
MICROPAPILLARY: Seen as complex bulbous protrusions WITHOUT fibrovascular cores
PAPILLARY: produces true papillae with fibrovascular cores AND lack myoepithelial layer
SOLID: Solid sheet of cells within the ducts or lobules confined by basement membrane.
MIXED: Mixture of two or more patterns as above.
Treatment: Mastectomy is curative in greater than 95% of women.
Chances of recurrece is high in the following conditions
a. hugh nuclear grade and necrosis
b.extensive disease
c. positive surgical margins.
Prognosis:If untreated, women with small, low-grade DCIS develop invasive cancer at a rate of about 1% per year. The risk increases with higher grades/extensive DCIS.
Lobular carcinoma in situ (LCIS)
Clonal proliferation of epithelial cells limited to ducts and lobules but the cells are DYSCOHESIVE which is its characteristic feature.
they are not associated with microcalcifications & stromal reactions and hence mammography might not be helpful in these cases.
why Dyscohesive??
because of loss of cell-cell adhesion resulting due to dysfunction of e-cadherin secondary to mutation of E Cadherin gene( CDH 1)
Morphology: the rells ar round ( lack of E-cadherin results in a rounded shape without attachment to adjacent cells ) uniform , with round or oval nuclei and a small nucleoli. Mucin positive signet ring cells are often present.
treatment and propgnosis: Bilateral prophylactic mastectomy, tamoxifen are considered as the risk of developing invasive carcinoma is high in either breast.
click here to read PATHOLOGY OF INFILTRATING DUCT CARCINOMA- BREAST https://ilovepathology.com/pathology-of-infiltrating-duct-carcinoma-breast/
click here to read PATHOLOGY OF MEDULLARY CARCINOMA- BREAST
{kind=link}