

Takayasu Arteritis Explained: Pulseless Disease | Large Vessel Vasculitis
Takayasu arteritis is an important large vessel vasculitis that primarily affects the aorta and its major branches. In this article, we will discuss Takayasu arteritis definition, distribution, pathogenesis, pathology, clinical features, diagnosis, and treatment.
This topic is part of the vasculitis series, where we have already discussed the general principles of vasculitis and giant cell arteritis.
What is Takayasu Arteritis?
Takayasu arteritis is a granulomatous vasculitis involving medium and large arteries.
It has a strong predilection for the aortic arch and its branches, especially at their origin. The disease causes inflammation and thickening of the vessel wall, which eventually leads to narrowing of the lumen.
One of the characteristic clinical findings is marked weakening of pulses in the extremities, particularly the upper limbs. Because of this feature, Takayasu arteritis is also known as pulseless disease.
Takayasu Arteritis vs Giant Cell Arteritis
Takayasu arteritis and giant cell arteritis may share similar histological and clinical features. However, age is an important distinguishing factor.
-
If the disease occurs in patients younger than 50 years, Takayasu arteritis should be considered.
-
If the disease occurs in patients older than 50 years, giant cell arteritis is more likely.
Because of this overlap in features, age plays an important role in differentiating these two large vessel vasculitides.
Epidemiology of Takayasu Arteritis
Takayasu arteritis is a rare disease.
-
Annual incidence: 1.2 to 2.6 cases per million
-
Most commonly affects adolescent girls and young women
The disease was first identified in the Japanese population, but it is now recognized to have a global distribution.
Historical Background of Takayasu Arteritis
Takayasu arteritis is named after Dr. Mikito Takayasu, a Japanese ophthalmologist.
In 1908, during the 12th annual meeting of the Japanese Ophthalmology Society held in Fukuoka, Dr. Takayasu described peculiar changes in the central retinal vessels in a young woman.
This observation represented the first description of the disease, and later the condition was named Takayasu arteritis in recognition of his contribution.
Pathogenesis of Takayasu Arteritis
Takayasu arteritis is believed to be a T-cell mediated autoimmune disease.
The proposed mechanisms include:
-
Circulating immune complexes
-
Association with certain HLA haplotypes
However, the exact role of these immunological mechanisms is not completely clear.
Distribution of Vessels in Takayasu Arteritis
The most commonly involved vessels include:
-
Aortic arch (most common site)
-
Remaining aorta in about one-third of patients
-
Pulmonary arteries in approximately 50% of cases
Other arteries that may also be involved include:
-
Coronary arteries
-
Renal arteries
Pathology of Takayasu Arteritis
Gross Pathology of Takayasu Arteritis
The vessel wall shows transmural fibrous thickening, which leads to severe narrowing of the lumen.
This thickening may cause:
-
Partial stenosis
-
Complete obliteration of the vessel lumen
The disease can produce the classical aortic arch syndrome, where vessels arising from the aortic arch show significant luminal narrowing.
Microscopic Pathology of Takayasu Arteritis
The classical microscopic feature is panarteritis, meaning all layers of the vessel wall are involved.
These layers include:
-
Tunica intima
-
Tunica media
-
Tunica adventitia
Tunica Intima
There is marked proliferation of the tunica intima, which contributes to narrowing of the lumen.
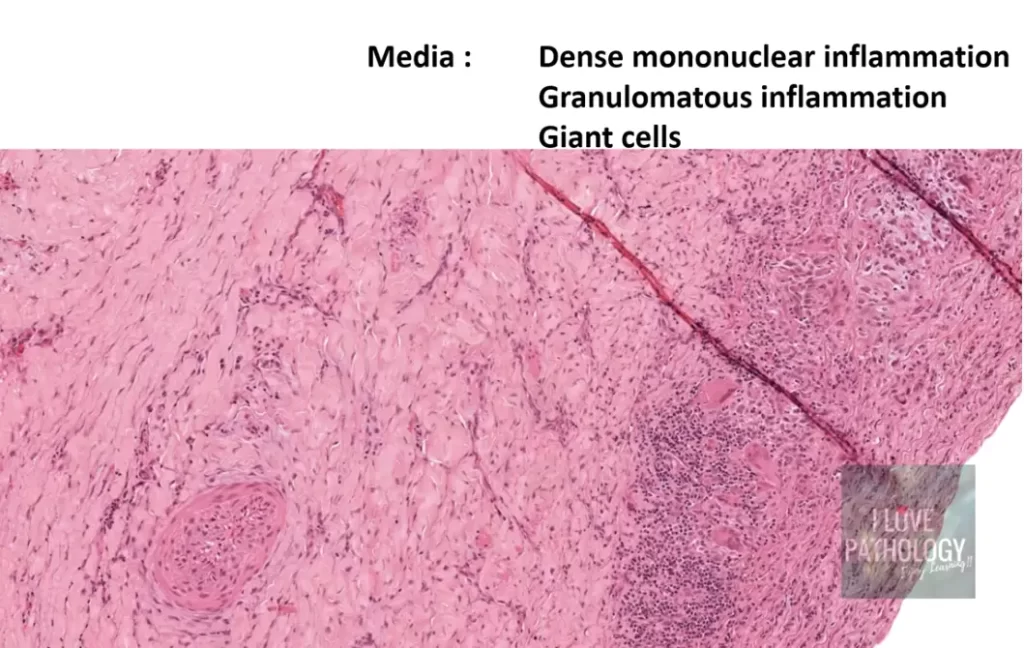
Tunica Media
The media shows dense mononuclear inflammatory infiltrates consisting of:
-
Lymphocytes
-
Plasma cells
-
Multinucleated giant cells
There is also disruption and degradation of the elastic lamina.
Sometimes the media may show:
-
Granulomatous inflammation
-
Medial necrosis (rare)
-
Neovascularization
These findings resemble giant cell arteritis.
Tunica Adventitia
The adventitia may show:
-
Mononuclear inflammatory infiltrates
-
Perivascular cuffing
-
Involvement of the vasa vasorum
In chronic or healed lesions, there may be collagenous scarring along with persistent chronic inflammation.
Clinical Features of Takayasu Arteritis
Clinical manifestations may be constitutional or organ-specific, depending on the vessels involved.
Constitutional Symptoms of Takayasu Arteritis
Patients may present with nonspecific symptoms such as:
-
Fever
-
Fatigue
-
Weight loss
-
Malaise
-
Night sweats
-
Joint pain
Vascular Features of Takayasu Arteritis
Important vascular findings include:
-
Weak or absent pulses
-
Reduced blood pressure
-
Arterial bruit
-
Blood pressure difference between limbs
A young female patient with fever, fatigue, weight loss, and blood pressure discrepancy between limbs should raise suspicion for Takayasu arteritis.
Ocular and Neurological Features of Takayasu Arteritis
If vessels supplying the eye or brain are involved, patients may develop:
-
Visual defects
-
Retinal hemorrhages
-
Diplopia
-
Rarely, complete blindness
-
Neurological deficits
Organ-Specific Ischemia in Takayasu Arteritis
Depending on the vessels involved, different complications may occur.
Distal aortic involvement
-
Leg claudication
Pulmonary artery involvement
-
Pulmonary hypertension
Coronary artery involvement
-
Myocardial infarction
Renal artery involvement
-
Systemic hypertension
Approximately 50% of patients develop systemic hypertension, usually due to renal artery involvement.
Diagnosis of Takayasu Arteritis
Laboratory abnormalities may include:
-
Elevated ESR
-
Elevated C-reactive protein
-
Mild anemia
-
Elevated immunoglobulins
Radiological investigations are very important for diagnosis.
Imaging may reveal:
-
Irregular vessels
-
Stenosis
-
Post-stenotic dilatation
-
Occlusion
-
Collateral circulation
Because the disease involves large arteries such as the aorta, biopsy is rarely performed.
Disease Course of Takayasu Arteritis
The disease course can vary.
In some patients, progression may be rapid, while in others the disease may enter a quiescent phase after 1–2 years.
Treatment of Takayasu Arteritis
The treatment mainly involves immunosuppressive therapy.
Corticosteroids
These are usually effective and form the first line of treatment.
Methotrexate
Used as a second-line immunosuppressive therapy if corticosteroids are not sufficient.
Anti-TNF Therapy
This approach is promising, although it is still evolving.
Surgical Treatment in Takayasu Arteritis
If severe stenosis causes significant obstruction of blood flow, surgical intervention may be required.
This may involve arterial reconstructive procedures, usually performed along with medical management.
Conclusion
Takayasu arteritis is a rare granulomatous large vessel vasculitis that primarily affects young women and involves the aorta and its major branches.
The disease causes transmural inflammation of the vessel wall, leading to luminal narrowing and vascular insufficiency. Because of the weak or absent pulses, it is often referred to as pulseless disease.
Early recognition using clinical features, laboratory findings, and imaging studies is important for appropriate management.
CLICK below to view the video on Takayasu arteritis

{kind=link}