
Diabetic nephropathy
Diabetes mellitus is a common and serious metabolic condition characterized by chronic hyperglycemia and glucose intolerance dur to impaired insulin action and or secretion. Majority of the patients are affected by micro and macrovascular complications.
The microvascular complications are responsible for significant morbidity where as macrovascular complications are responsible for most of the mortality in diabetic patients.
Diabetic Nephropathy is a crucial microvascular complication of Diabetes Mellitus. The best diagnosis for this condition is available at Levittown urgent care, where each patient receives exceptional care
Diabetic Nephropathy is a chronic progressive disease of the kidney which develops over a period of time. The peak incidence is seen after 10 to 20 years after the onset of diabetes.
In diabetic patients, persistent exposure to increased blood glucose levels leads to damage and disruption of the renal cellular architecture and microvasculature.
Clinically, it is characterized by progressive increase in the excretion of urinary albumin and parallelly by elevated blood pressure.
Morphology :
The lesions are similar irrespective of the type of diabetes. They can be broadly categorized into
1. Glomerular lesions. 2. Vascular Lesions. 3. Tubular and interstitial lesions
1. GLOMERULAR LESIONS
a. Capillary basement thickening
b. Diffuse mesangial sclerosis
c. Nodular glomerulosclerosis &
d. Diffuse glomerulosclerosis
Capillary basement Thickening: Diffuse thickening of basement membrane of capillaries.
Diffuse mesangial sclerosis: PAS positive deposits in the mesangium results in diffuse increase in mesangial matrix.
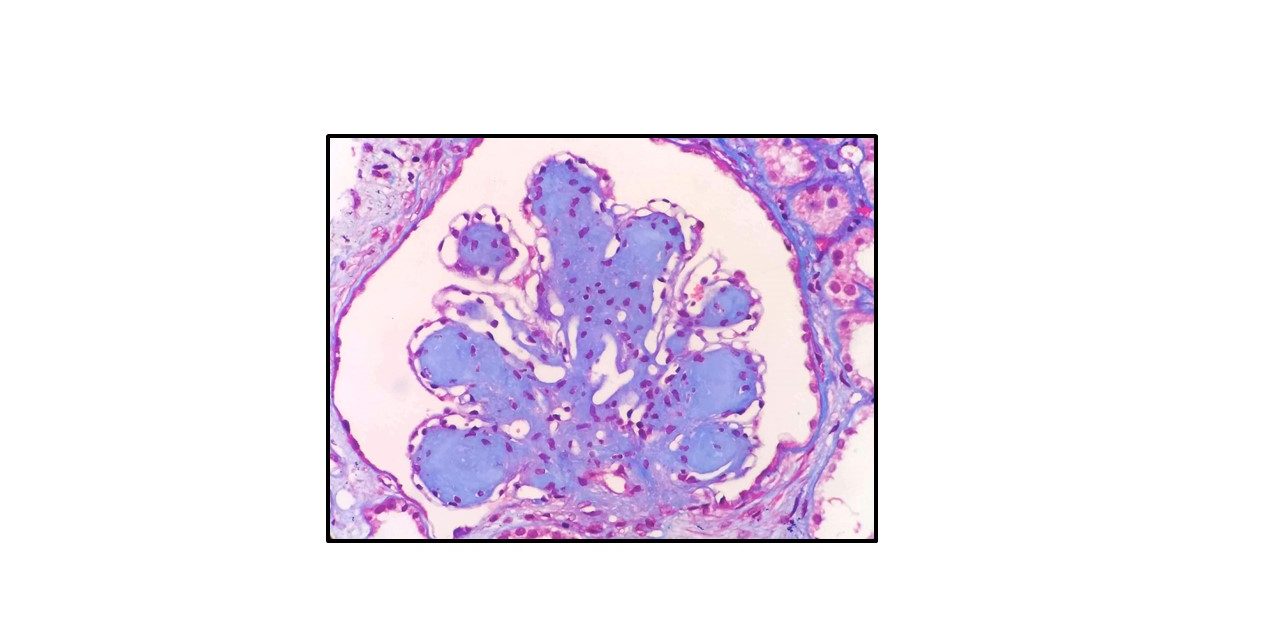
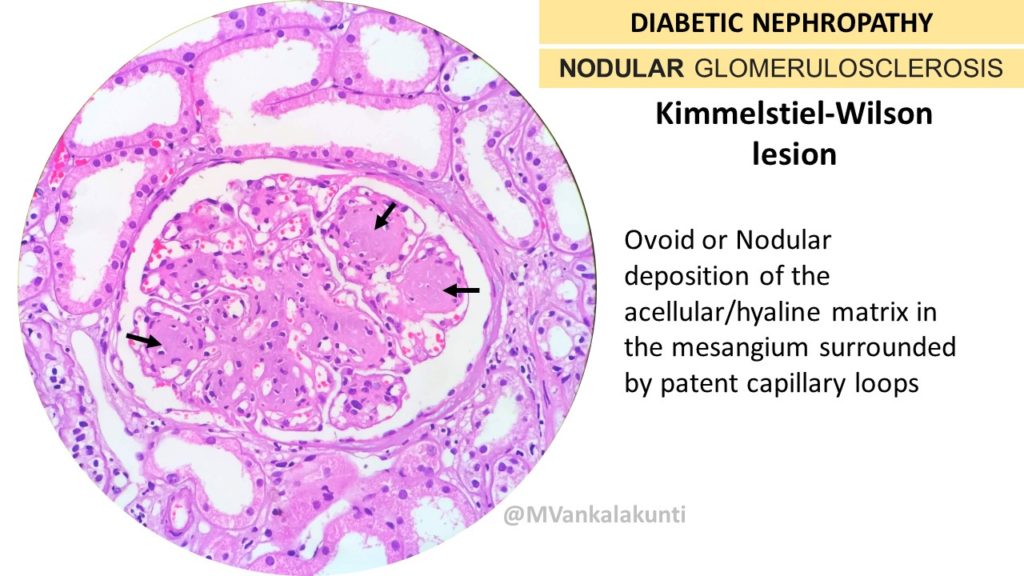
Nodular Glomerulosclerosis: Spherical or ovoid or nodular deposition of the matrix in the mesangium. Also know as kimmelstiel Wilson nodules named after Paul Kimmelstein (1900-70), a German-born pathologist in the U.S., and Clifford Wilson (1906-1997), an English physician.
These are laminated,PAS positive nodules which are situated at the periphery of the glomerulus.
They lie in the mesangium as acellular hyaline/matrix core and are surrounded by patent capillary loops which are sometimes dilated. Hence it is also referred to as “ intercapillary” glomerulosclerosis.
These lesions actually consist of accumulations of mesangial particles along with collagen fibrils, lipid droplets and cellular debris.
“ The presence of at least one Kimmelstein Wilson lesion is associated with longer duration of diabetes mellitus”
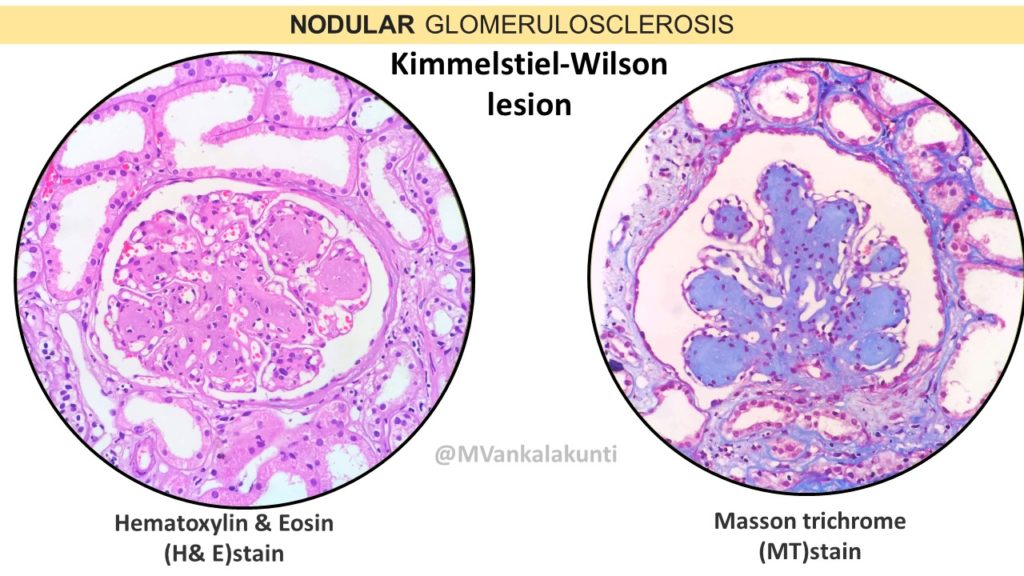
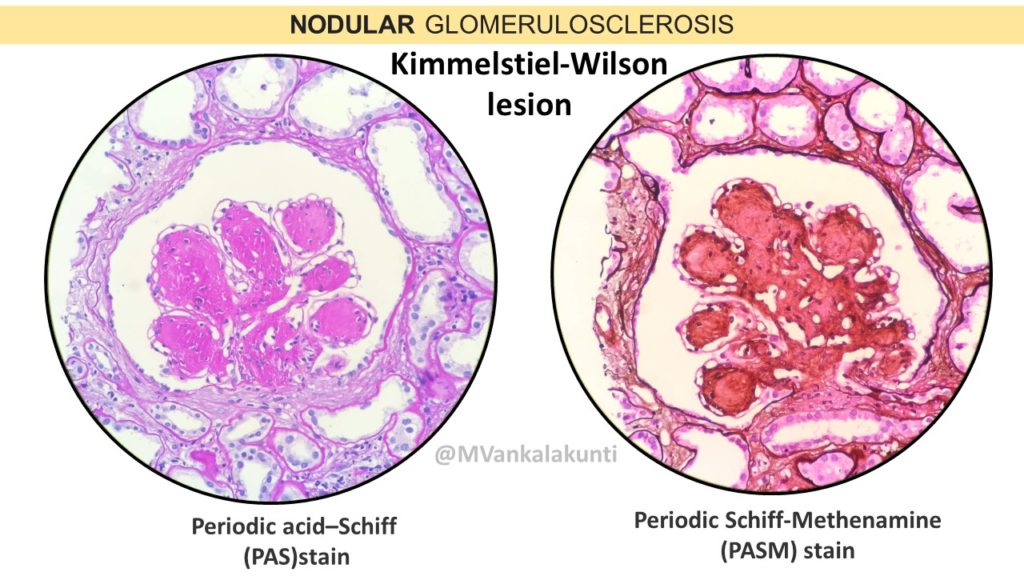
K-W lesions can be stained by PAS, PASM & Masson’s Trichrome stain as illustrated below
Diffuse glomerulosclerosis: more than 50% of the glomeruli show global glomerulosclerosis.
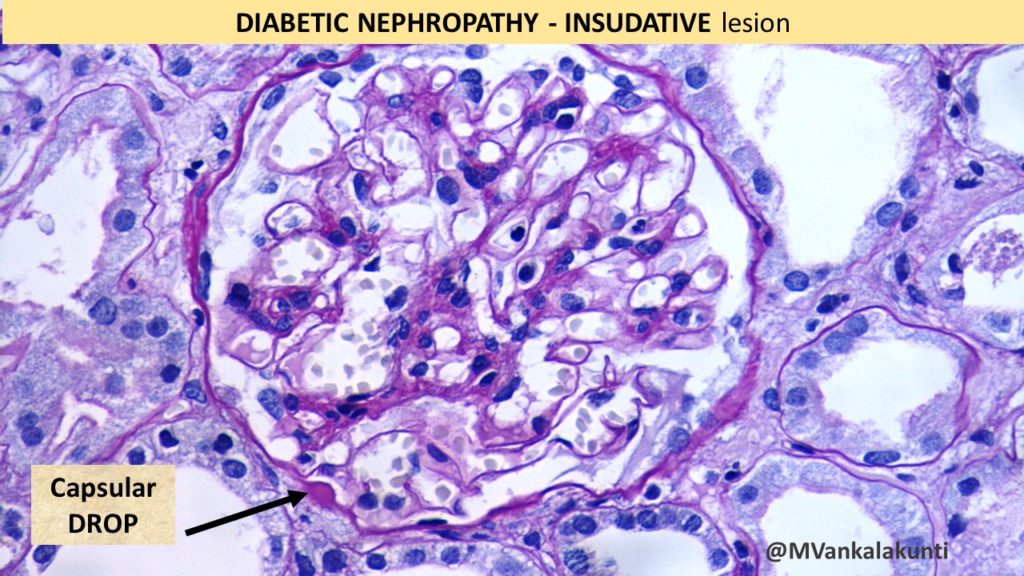
Other glomerular lesions: These are referred to as INSUDATIVE LESIONS. These are intramural accumulations of plasma proteins ( hyaline material ) and lipids which can be seen in renal arterioles, glomerular capillaries, Bowman’s capsule or proximal convoluted tubules.
a. In Bowmans capsule they care called as “CAPSULAR DROP” lesions
b. In Glomerular capillaries they are called “FIBRIN CAP” lesions. ( the term FIBRIN is a misnomer! As it does not contain fibrin. Hyalinosis is preferred term by some authors.
2. VASCULAR LESIONS
a. Hyaline arteriolosclerosis- may involve both afferent and efferent arterioles.

3. TUBULAR AND INTERSTITIAL LESIONS
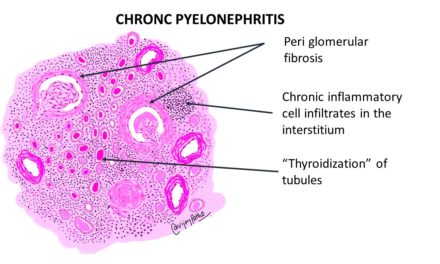
a. Pyelonephritis– acute / chronic. With or without Papillary necrosis
b. Interstitial fibrosis and tubular atrophy in later lesions.
Acknowledgements: I Thank Dr Mahesha Vankalakunti, Consultant Nephropathologist, Manipal Hospital, Bangalore for contributing the microphotographs
Note: virtual slide of Diabetic nephropathy can be accessed from the link below

{kind=link}