
PLASMA CELL NEOPLASMS
Introduction: Plasma cell neoplasms result from clonal expansion of terminally differentiated B cells that secrete monoclonal immunoglobulin called ‘M’ protein. These include:
Plasma cell myeloma
Plasmacytoma
Monoclonal immunoglobulin deposition disease
Plasma cell neoplasm associated with paraneoplastic syndrome
How are immunoglobulins formed?
Ever wondered how our body fights against diseases? We fall sick and then recover eventually. All credit goes to our immune system and mainly B lymphocytes. B cells arise in the bone marrow which is primary lymphoid organ (hence the term ‘B’) and then migrates to secondary lymphoid organs like spleen and lymph node where further development occurs. When there is suitable antigenic stimulation, the B Cells differentiate in to plasma cells that secrets antibodies which are polyclonal in nature and cause destruction of target cells/ organisms.

“Abnormal proliferation of these plasma cells results in plasma cell neoplasm/plasma cell dyscrasias. They are also called paraproteinemia or monoclonal gammopathies”
What do you mean by the term M protein?
Immunoglobulins or antibodies are made up of two identical heavy chains(H) and two identical light chains(L). Heavy chains are α,δ,ε,ϒ,µ and accordingly we have immunoglobulins IgA, IgD, IgE, IgG and IgM. Light chains are of two varieties- kappa(κ) and lambda (λ)
M protein refers to the presence of homogenous protein in serum or urine detected by electrophoresis and are synthesized by monoclonal plasma cells. These proteins may be complete immunoglobulin molecules of same class or can be light chains of same type or may be heavy chain of same class
MULTIPLE MYELOMA
What is multiple myeloma?
It is a plasma cell neoplasm characterized by monoclonal proliferation of plasma cells associated with lytic bone lesions, hypercalcemia, renal failure, and acquired immune abnormalities. Bone marrow shows numerous plasma cells.
Pathogenesis:
It is associated with frequent rearrangements involving IgH locus and various proto-oncogenes.
Clinical features:
The clinical features are well remembered with acronym CRAB as illustrated in the figure below

Morphology
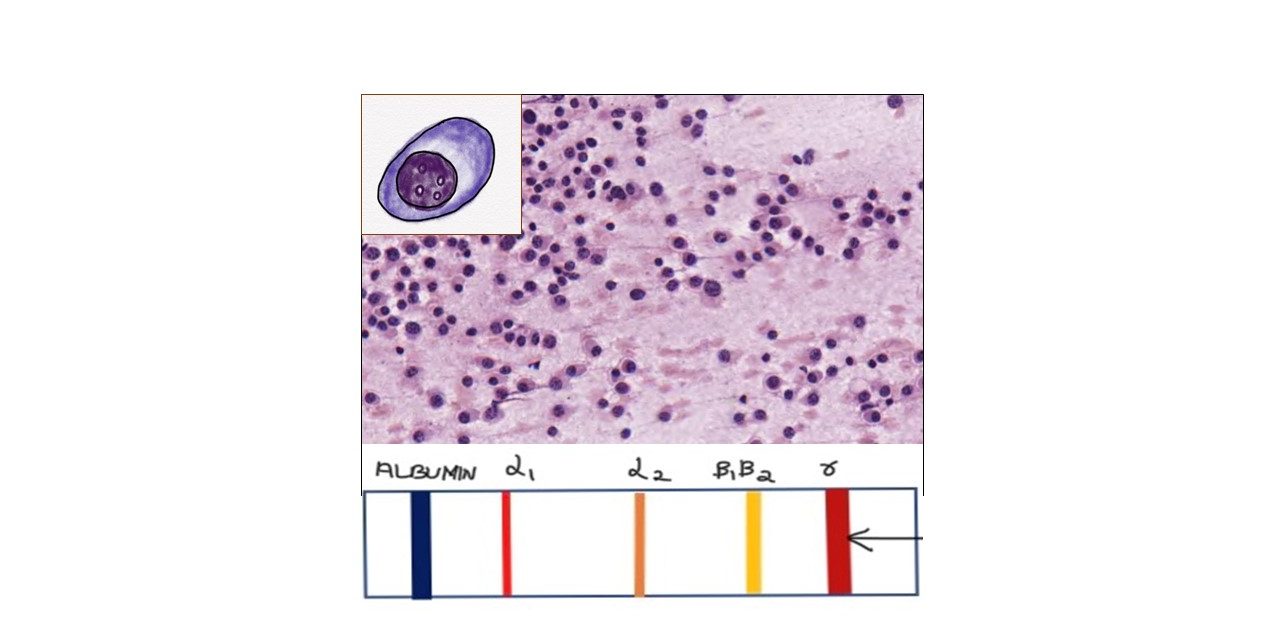
Bone marrow shows increased plasma cells as shown in the figure
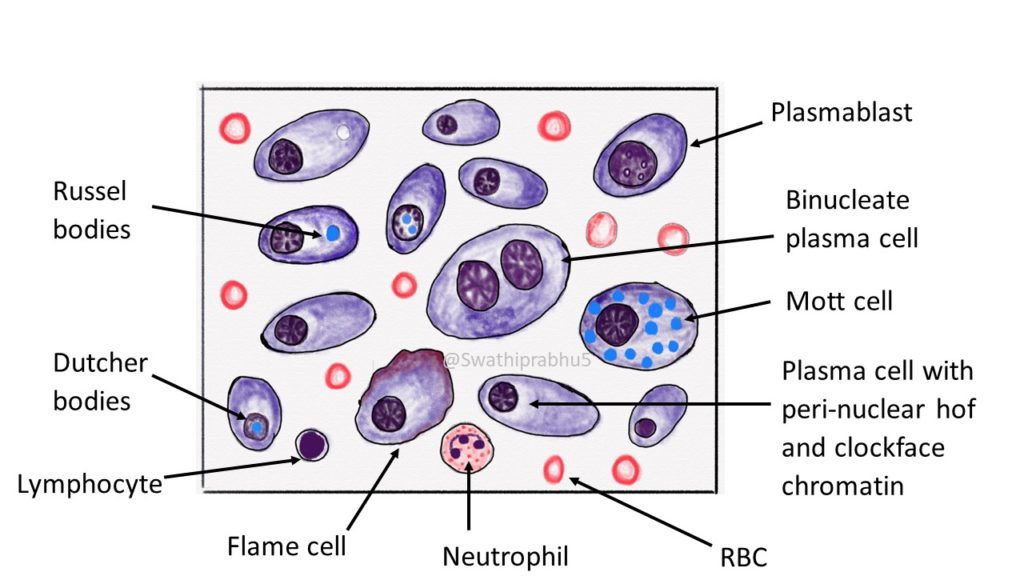
Plasma cells: They are oval to round shaped with eccentrically placed nucleus, clockface chromatin, basophilic cytoplasm and characteristic perinuclear hof (pale staining area corresponding to golgi region of plasma cell). Immature plasma cells and plasmablasts are also seen.
Plasmablasts: They are large cells with high nuclear to cytoplasmic ratio, fine reticular nuclear chromatin and prominent nucleoli.
Russel bodies: These are cytoplasmic inclusions seen in plasma cells composed of immunoglobulins. They stain pale blue in Leishman stain and eosinophilic in Hematoxylin and eosin stain( as illustrated below). When multiple inculsions are seen in a plasma cell, then it is called as mott cell.

Dutcher bodies: Intranuclear inclusions in a plasma cell are known as dutcher bodies
Flame cells: sometimes cytoplasm may show flaming with peripheral free border showing orange-red colour. Such cells are glycogen rich and IgA secreting.
Investigations:
To evaluate for M protein
1) Serum protein electrophoresis:
The M protein which is secreted by plasma cells can be detected by serum or urine electrophoresis.
The principle behind this technique is to separate different proteins on the basis of their charge. Here, the serum is applied to the supporting medium and is then placed in electrophoresis chamber containing alkaline buffer solution. Electric current is passed and the proteins are separated based on their charge.

2) Urine electrophoresis
3) Immunofixation: Preferred method which helps in identification of M protein
4) Bence jones proteinuria:
They are monoclonal immunoglobulin light chains(κ or (λ) synthesized monoclonal plasma protiens. They have characteristic behaviour. When heated, Bence jones proteins precipitate at temperature between 40 to 60 degree Celsius and precipitate disappears on further heating at 85-100 degree Celsius and reappears on cooling.
5) Quantification of Monoclonal immunoglobulins
6) Radiological studies. The lesions are seen as small,numerous, well-circumscribed, lytic/ punched-out lesions within the skull, vertebrae, and pelvis. these findings on the skull is also referred to as “Raindrop skull”
( describing the lesion which resembles like rain hitting the surface and splashing, leaving behind random spots)


{kind=link}