
Myocardial infarction (MI):why is it important to study its gross and microscopic changes?
Myocardial infarction (MI) occurs due to the obstruction of coronary arteries, leading to ischemia and necrosis of heart muscle. Understanding its gross and microscopic changes helps predict the time since infarction, assess complications, and correlate with clinical outcomes.
Nearly all transmural infarcts involve a portion of the left ventricle, including the free wall and ventricular septum. The infarct typically covers the entire perfusion zone except for a narrow subendocardial rim (about 0.1 mm), which is preserved due to diffusion of oxygen from the blood within the heart chambers.
Which arteries are commonly involved in myocardial infarction?
Left anterior descending (LAD) artery (40–50%): Infarcts affect the anterior left ventricular wall (especially at the apex), anterior ventricular septum, and apex circumferentially.
Right coronary artery (30–40%): Infarcts affect the inferior or posterior left ventricular wall, posterior ventricular septum, and sometimes the posterior right ventricular free wall.
Left circumflex artery (15–20%): Infarcts affect the lateral left ventricular wall, except for the apex.
Infarcts can also arise from obstructions in the left main coronary artery, diagonal branches of the LAD, or marginal branches of the left circumflex artery. Isolated right ventricular infarcts are rare (1–3% of cases).
How do myocardial infarcts appear grossly and microscopically at different time intervals?
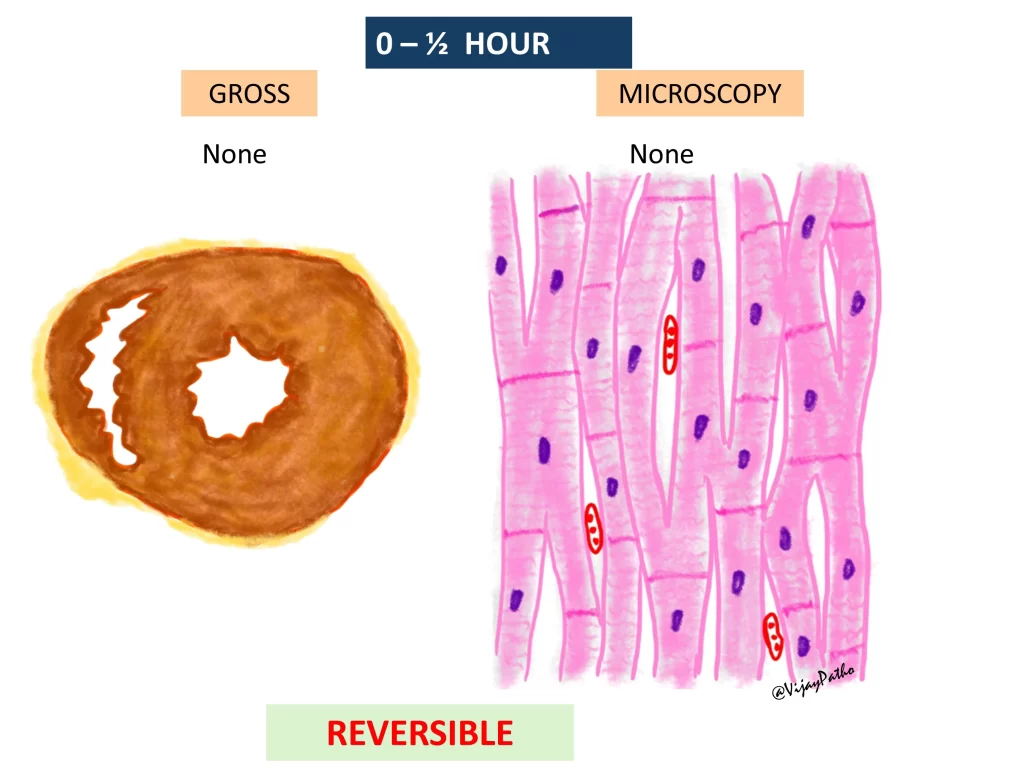
0–30 minutes:
Grossly: No visible changes.
Microscopically: No significant changes under light microscopy. On electron microscopy, there may be relaxation of myofibrils, glycogen loss, and mitochondrial swelling (features of reversible injury).
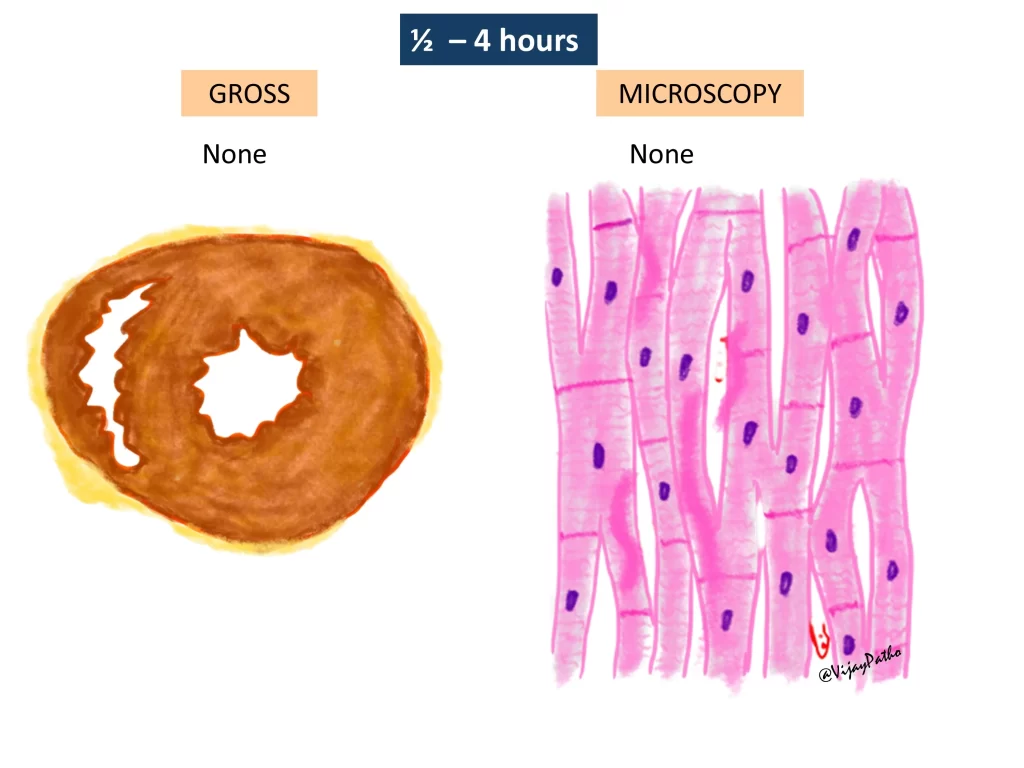
30 minutes–4 hours:
Grossly: No visible changes.
Microscopically: Waviness of myocardial fibers may be seen. On electron microscopy, sarcolemmal disruption and mitochondrial amorphous densities appear.
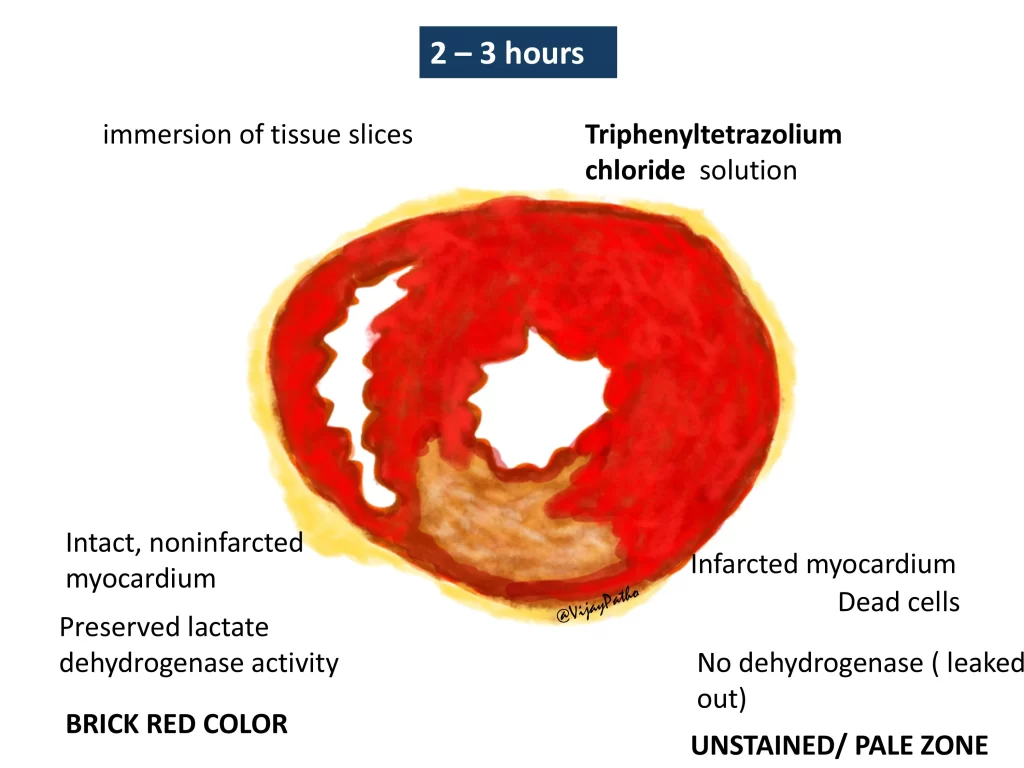
Special stain (Triphenyl Tetrazolium Chloride test): Non-infarcted myocardium stains brick red, while infarcted tissue appears pale due to loss of lactate dehydrogenase enzyme.
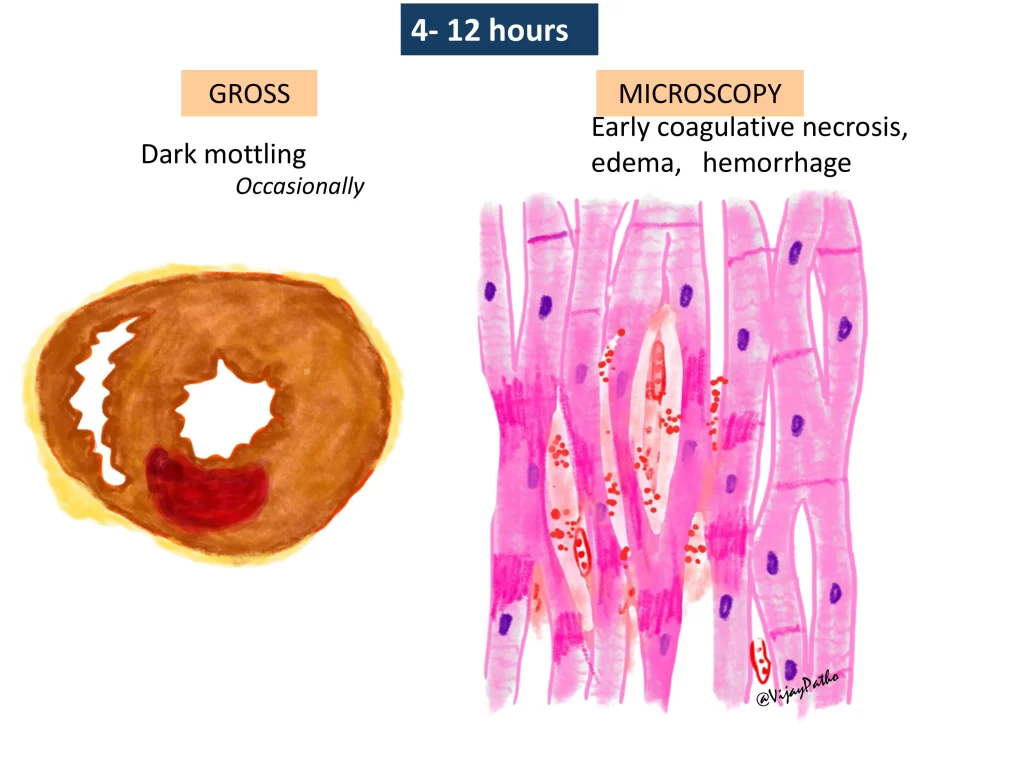
4–12 hours:
Grossly: Occasional mottling (red discoloration due to hemorrhage).
Microscopically: Early coagulative necrosis begins, with cytoplasmic eosinophilia (cells become more pink) and nuclear fading. Contraction band necrosis may be seen.
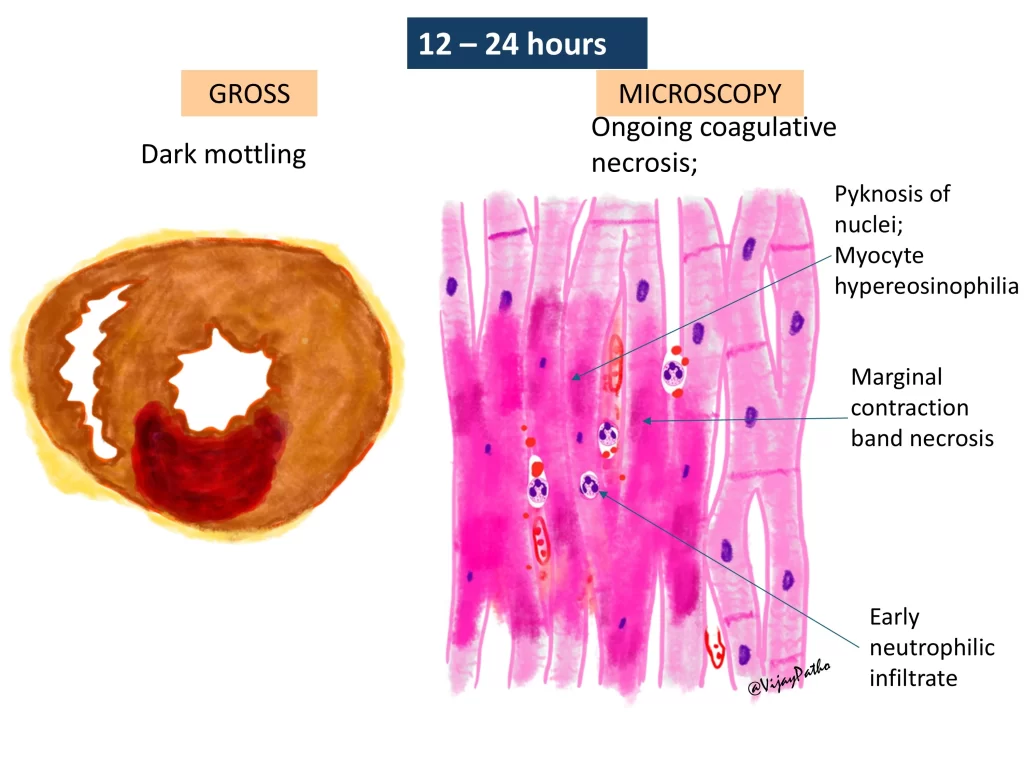
12–24 hours:
Grossly: Mottling increases.
Microscopically: Well-formed coagulative necrosis, pyknosis of nuclei, myocyte hyper-eosinophilia, and early neutrophilic infiltrate. Hemorrhage may be present.
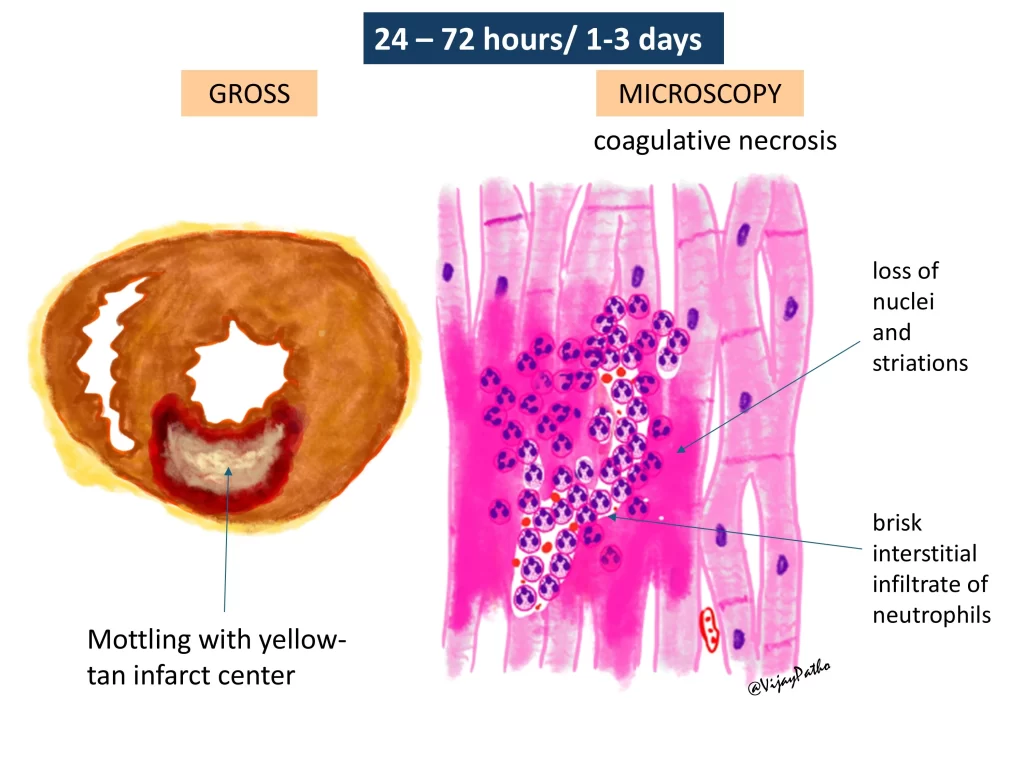
1–3 days:
Grossly: Mottling with a yellow-tan center.
Microscopically: Extensive coagulative necrosis, complete loss of nuclei, and heavy neutrophilic infiltration.
Clinical relevance: Risk of pericarditis if untreated.
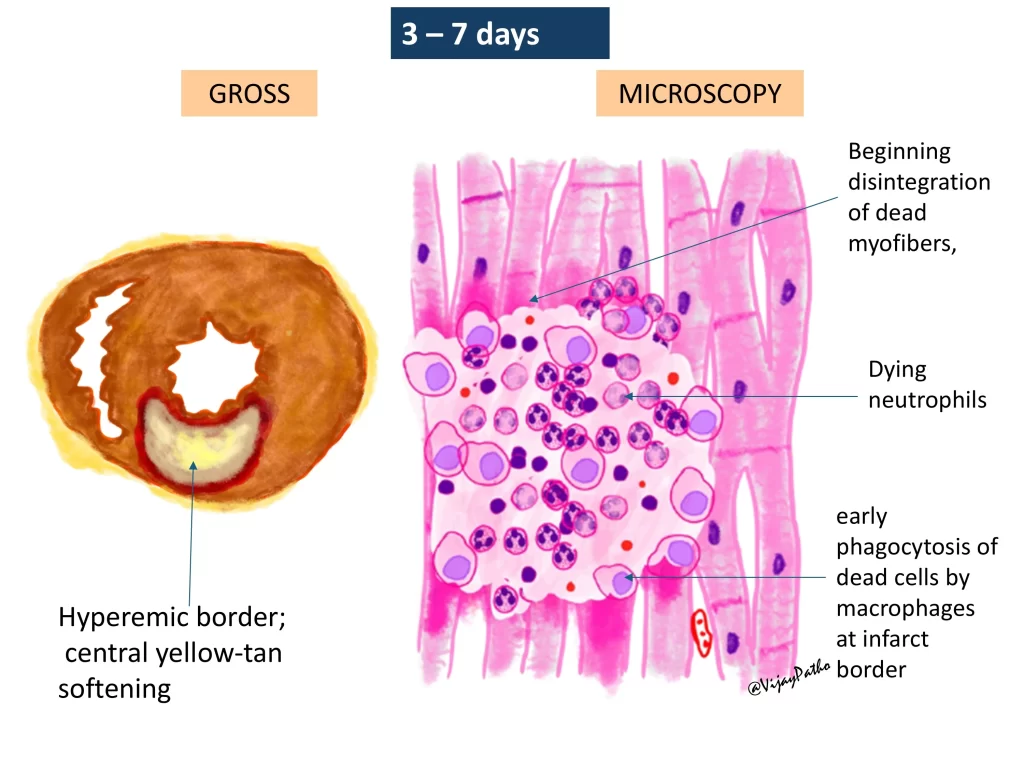
3–7 days:
Grossly: Hyperemic borders, softening of infarcted tissue.
Microscopically: Beginning of myocyte disintegration, peak neutrophilic infiltration, and appearance of macrophages clearing debris.
Clinical relevance: Risk of ventricular wall rupture due to tissue weakening.
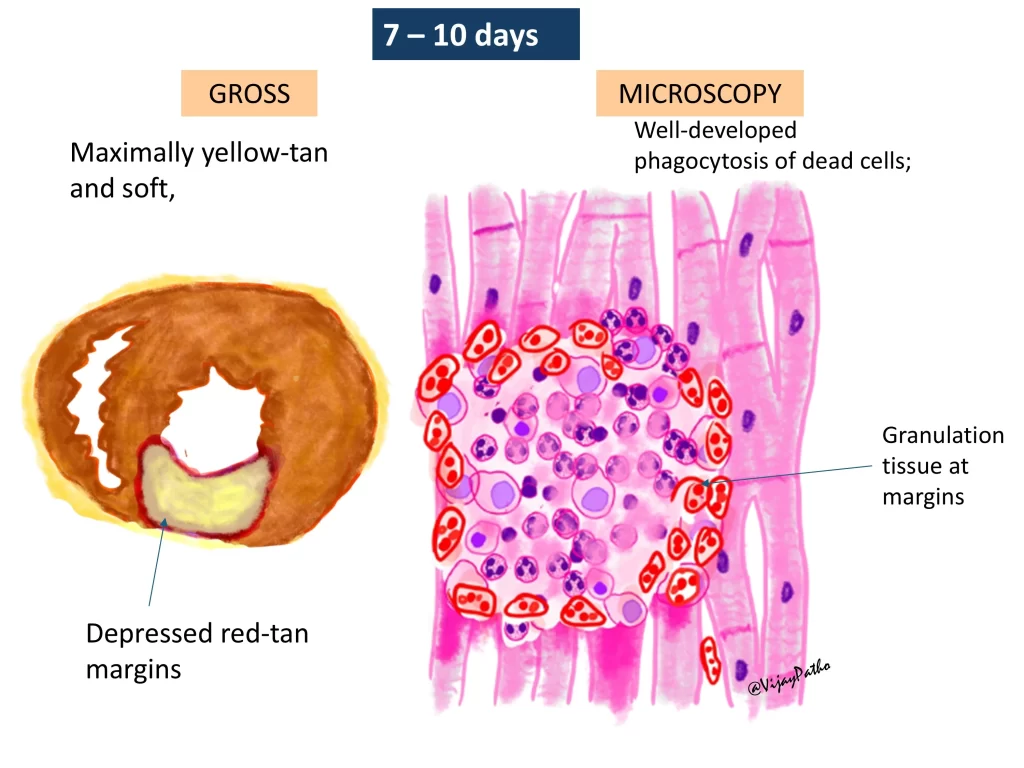
7–10 days:
Grossly: Maximally yellow-tan infarct, very soft, with depressed red-tan margins (granulation tissue formation).
Microscopically: Prominent macrophage activity, phagocytosis of dead cells, and proliferation of granulation tissue with capillary ingrowth.
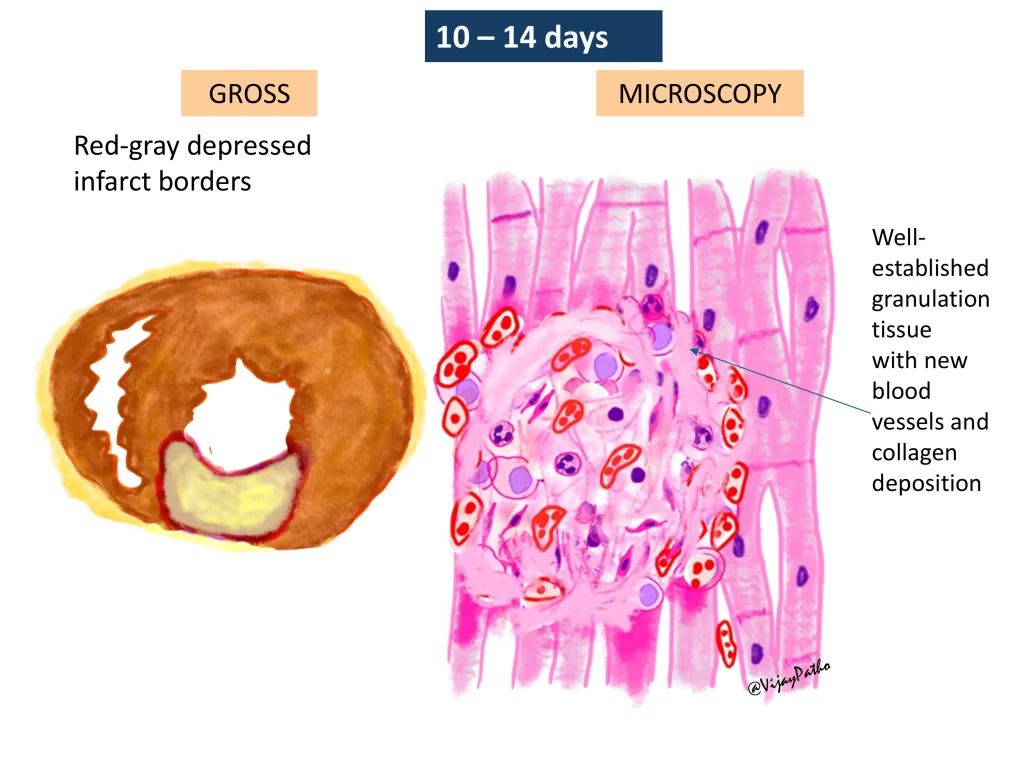
10–14 days:
Grossly: Red-gray infarct borders, persistent yellowish center.
Microscopically: Well-established granulation tissue with early collagen deposition.
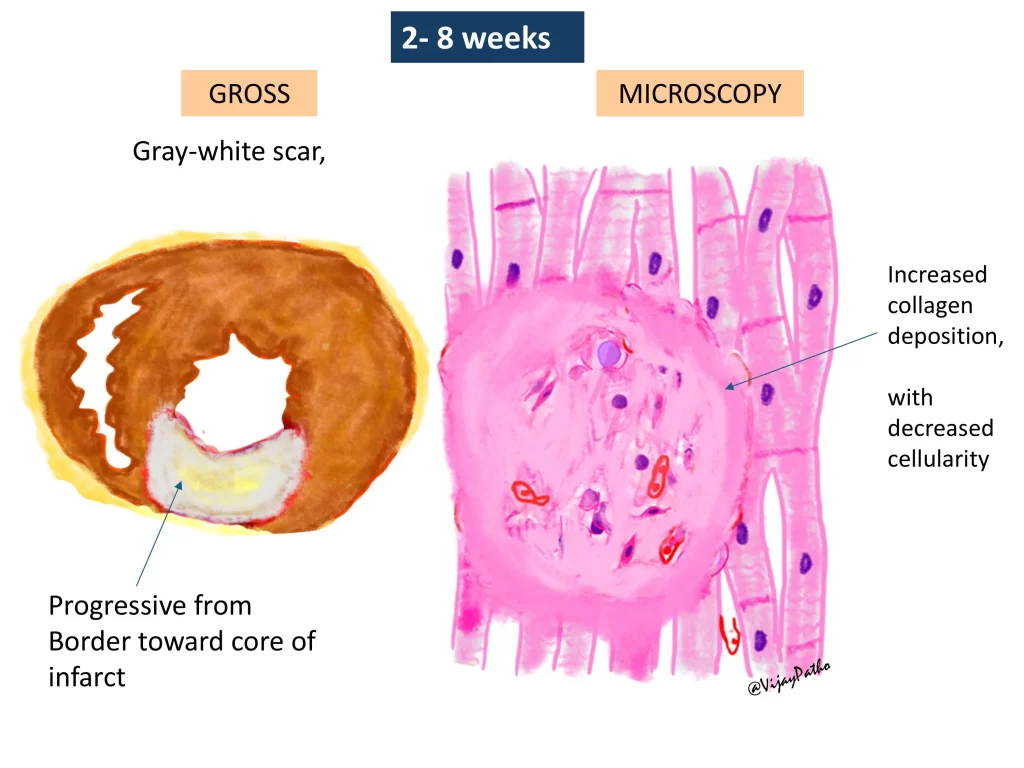
2–8 weeks:
Grossly: Formation of a gray-white scar, which progressively moves from the periphery toward the center.
Microscopically: Increased collagen deposition, reduced cellularity.
Beyond 2 months:
Grossly & Microscopically: Complete scar formation with dense collagen. The appearance remains the same even after several years.

Why is it important to study the sequence of myocardial infarction changes?
Understanding these changes helps in estimating the time since infarction, predicting complications, and determining the cause of death in autopsies. Each stage correlates with specific clinical risks:
1–3 days: Increased risk of pericarditis.
3–7 days: Risk of myocardial rupture due to softening of the infarcted area.
7–10 days onward: Granulation tissue and collagen deposition start, indicating the beginning of scar formation.
Watch the video tutorial in the link below


{kind=link}