
Essential Thrombocythemia (ET)
Essential thrombocythemia is a myeloproliferative neoplasm characterized by sustained thrombocytosis. The key pathological feature is an increased number of large, mature megakaryocytes in a normally cellular bone marrow.
Some textbooks may use the term essential thrombocytosis, but the correct and preferred term is essential thrombocythemia.
How common is Essential Thrombocythemia and who gets it?
The incidence of essential thrombocythemia is around 1 to 3 cases per 100,000 population, similar to polycythemia vera.
It most commonly affects individuals above 60 years of age, but it can also occur in younger patients.
What is the pathogenesis of Essential Thrombocythemia?
About 90% of cases of essential thrombocythemia have mutations that result in increased JAK-STAT signaling.
A simple mnemonic to remember the mutations is “JAK might C”:
-
J – JAK2 mutation
-
M – MPL mutation
-
C – CALR mutation
The distribution of mutations is as follows:
-
JAK2 mutation: seen in about 50–60% of cases
-
MPL mutation: seen in about 5–10% of cases
-
CALR mutation (calreticulin): seen in around 30% of cases
All these mutations ultimately lead to overactivation of the JAK-STAT pathway.
Interestingly, even though the JAK2 mutation is also seen in polycythemia vera, we still do not clearly understand why some patients develop essential thrombocythemia while others develop polycythemia vera.
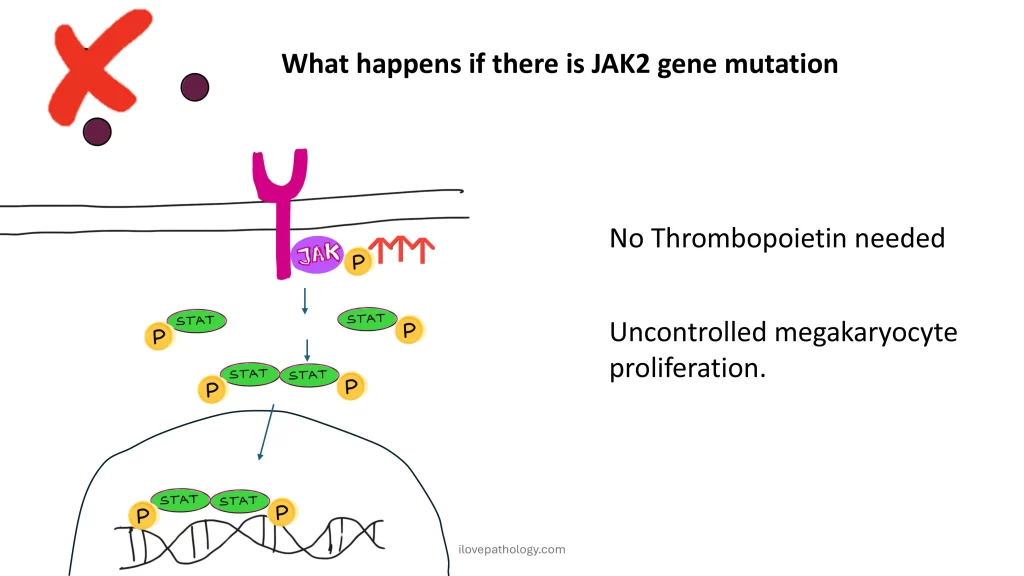
How does the JAK-STAT pathway lead to thrombocytosis?
Normally, a growth factor such as thrombopoietin binds to its receptor on the hematopoietic stem cell. This activates the JAK kinase, which then activates STAT proteins. These STAT proteins dimerize, enter the nucleus, and activate genes responsible for megakaryocyte production.
In essential thrombocythemia, due to mutations in JAK2, MPL, or CALR, this pathway becomes constitutively active, meaning:
-
Thrombopoietin is not required
-
There is uncontrolled proliferation of megakaryocytes
-
This results in persistent thrombocytosis

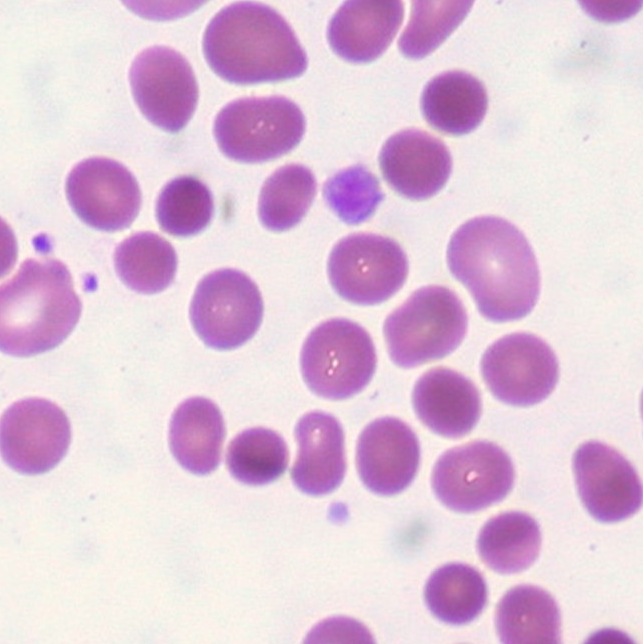
What are the peripheral blood smear findings in Essential Thrombocythemia?
The peripheral smear shows:
-
Thrombocytosis, usually more than 4.5 lakh platelets per cubic millimeter
-
Large and giant platelets
-
Occasionally hypogranular platelets
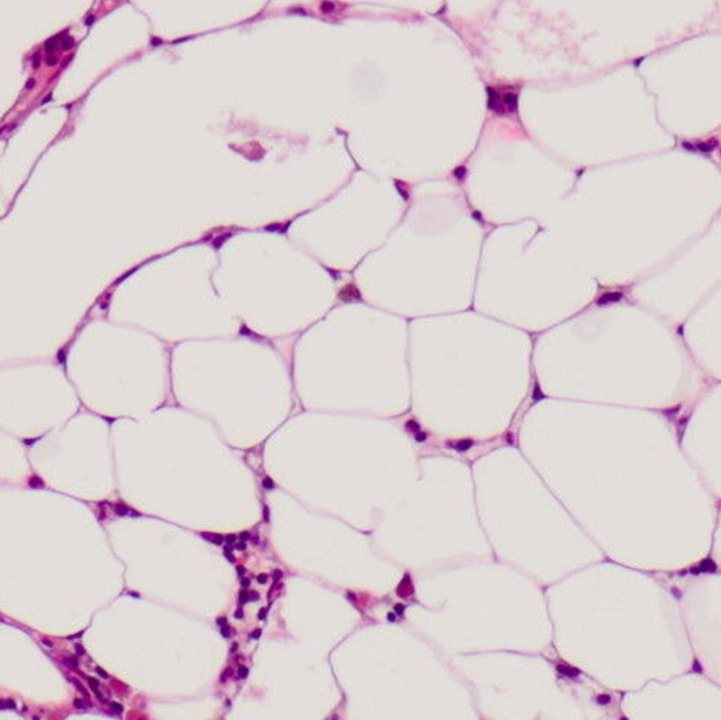
What are the bone marrow findings in Essential Thrombocythemia?
The bone marrow is usually normocellular for the age of the patient, though mild increase in cellularity may be seen.
The most striking feature is:
-
Marked proliferation of megakaryocytes
These megakaryocytes show:
-
Large to giant forms
-
Irregular size and shape
-
Abundant mature cytoplasm
-
Deeply lobulated or hypersegmented nuclei, sometimes described as staghorn-like
Importantly, there are no dysplastic features.
The presence of dysplasia should always raise suspicion for myelodysplastic neoplasms, not myeloproliferative neoplasms.
Delicate reticulin fibrosis may be present, but it is not as prominent as in polycythemia vera.
Mild splenomegaly may occur due to extramedullary hematopoiesis.
Why do patients with Essential Thrombocythemia develop symptoms?
Although the platelet count is high, most platelets are functionally abnormal because they arise from a neoplastic clone.
As a result, patients develop:
-
Thrombosis
-
Hemorrhage
What are the thrombotic manifestations of Essential Thrombocythemia?
Thrombotic complications are similar to those seen in polycythemia vera and include:
-
Deep vein thrombosis
-
Myocardial infarction
-
Stroke
-
Hepatic vein thrombosis leading to Budd–Chiari syndrome
-
Portal or mesenteric vein thrombosis, which may cause bowel infarction
What bleeding manifestations are seen in Essential Thrombocythemia?
Bleeding manifestations are usually mild and include:
-
Epistaxis
-
Bleeding gums
Severe or life-threatening hemorrhage is rare in essential thrombocythemia.
How is Essential Thrombocythemia diagnosed?
The diagnosis is based on major and minor criteria.
The major criteria include:
-
Platelet count greater than 4.5 lakh
-
Bone marrow biopsy showing megakaryocytic proliferation with normal erythroid and granulocytic lineages
-
Absence of features of other myeloproliferative neoplasms such as:
-
BCR-ABL positive CML
-
Polycythemia vera
-
Primary myelofibrosis
-
-
Presence of JAK2, CALR, or MPL mutation
The minor criterion includes:
-
Presence of a clonal marker
or -
Exclusion of reactive causes of thrombocytosis
Diagnosis can be made when:
-
All four major criteria are present, or
-
First three major criteria plus one minor criterion are fulfilled
How is Essential Thrombocythemia treated?
Treatment aims to reduce platelet production and prevent complications.
Commonly used therapies include:
-
Hydroxyurea – the most commonly used first-line drug
-
Anagrelide – selectively reduces platelet production, preferred in younger patients and pregnant women
-
Interferon-alpha – modulates immune response and reduces megakaryocyte proliferation
What is the prognosis of Essential Thrombocythemia?
Essential thrombocythemia is a slow-growing and indolent disorder.
Patients may remain asymptomatic for long periods.
Compared to other myeloproliferative neoplasms, the prognosis is better, with a median survival of around 12–15 years.
Thrombotic complications are more common in patients with homozygous mutations, where both gene copies are affected.
CLICK BELOW to watch the video tutorial on Essential thrombocythemia


{kind=link}