
What is Cutaneous Squamous Cell Carcinoma?
• Malignancy of epidermal keratinocytes with variable degrees of differentiation and cytological features
Sites
• Most often in sun exposed areas
• Incidence: 5 – 499 per 1,000 individuals depending on the latitude
• Scalp, ear, lip, nose, eyelid are high risk anatomic sites
Etiology
• Chronic ulcers
• Chronic inflammation
• Sinus tract
• Human papillomavirus infection
• Tars / oils
• Xeroderma pigmentosa
• Ultraviolet light radiation and other forms of radiation
• Chronic immunosuppression
• Actinic keratosis (precursor lesion)
• Albinism (lack of pigmentation in skin), arsenic
• Burn scars

Pathophysiology
• Multistep pathway including damage through UV radiation, mutations involving genes (such as TP53, CDKN2A) and molecular pathways (RAS / RAF)
Clinical features
• Erythematous scaly thin papule or plaque
Prognostic factors
• Depends on a few factors:
1. diameter: > 2 cm, 2x risk of recurrence, 3x rate of metastasis
2. depth: > 2 mm, 10x risk of local recurrence
3. perineural invasion: involved nerves ≥ 0.1 mm, increased nodal metastases
4. poor differentiation indicates poor prognosis
5. lymphovascular invasion
6. high risk anatomic sites (scalp, ear, lip, nose, eyelid)
Staging
• Based on lesion size, depth of invasion, differentiation and perineural invasion
• AJCC, eighth edition of the American Joint Committee on Cancer for cutaneous squamous cell carcinoma of the head and neck
• pT1: Tumor diameter ≤ 2 cm
• pT2: Tumor diameter ≥ 2 cm and < 4 cm
• pT3: Tumor with diameter ≥ 4 cm or with one of the high risk features
• pT4a: Tumor with gross cortical bone / marrow invasion of maxilla, mandibular orbit or temporal bone
• pT4b: Tumor with skull base invasion or skull base foramen involvement
High risk features: perineural invasion (of a nerve lying beneath the dermis or ≥ 0.1 mm in caliber or presenting with clinical or radiographic involvement of named nerves without skull base invasion or transgression), deep invasion (involvement beyond the subcutaneous fat or > 6 mm) and minor bone erosion
Treatment
• Mohs surgery: excision with adequate margins
• Curettage, cryotherapy, radiation therapy
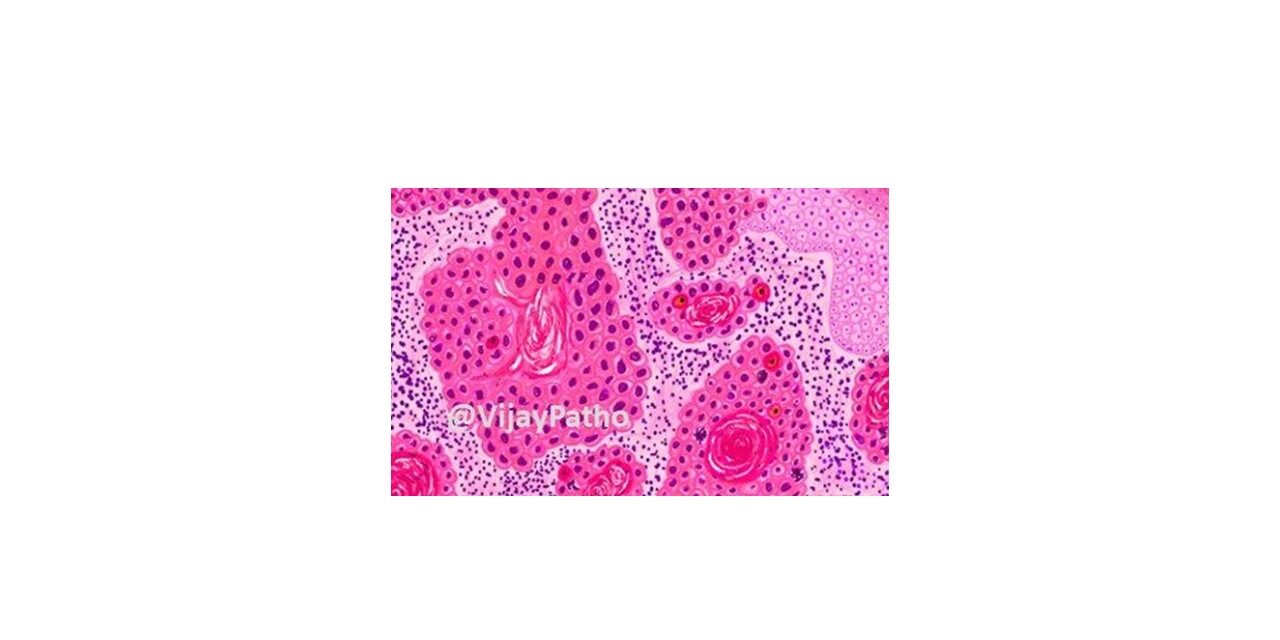
Microscopic (histologic) description
• Carcinoma of keratinocytes that infiltrates the dermis
• Precursor lesion (actinic keratosis / dysplasia / squamous cell carcinoma in situ) is often present
• Downward growth below level of adjacent or overlying epidermis
• Grading is evaluated on the basis of differentiation and keratinization
• Malignant cells are large with abundant eosinophilic cytoplasm and a large, often vesicular, nucleus
Positive stains
• Keratins: AE1 / AE3, CK5/6, CK5
• EMA
• p63, p40
References
• Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders
• Yanofsky VR, Mercer SE, Phelps RG. Histopathological variants of cutaneous squamous cell carcinoma: a review. J Skin Cancer. 2011;2011:210813.

{kind=link}