
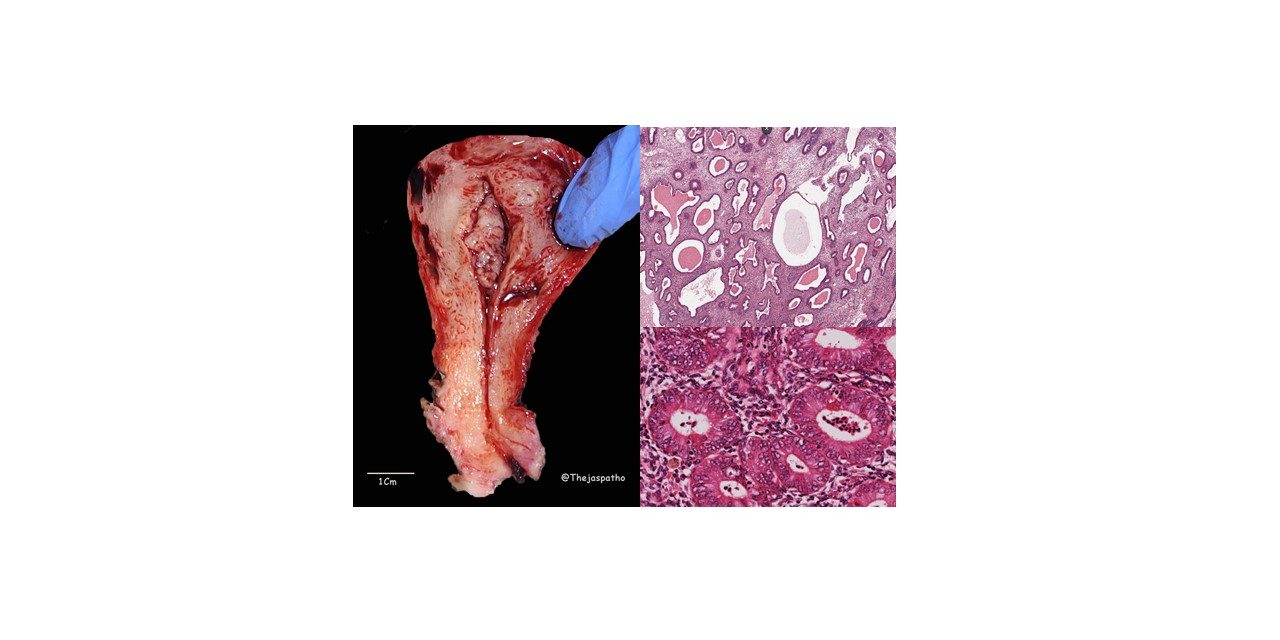
ENDOMETRIAL HYPERPLASIA
Definition: is defined as an abnormal proliferation of the endometrial glands relative to the stroma, resulting in an increased gland-to-stroma ratio
Most common symptom: Abnormal vaginal bleeding
Precursor lesion for Endometrial Carcinoma, endometroid type
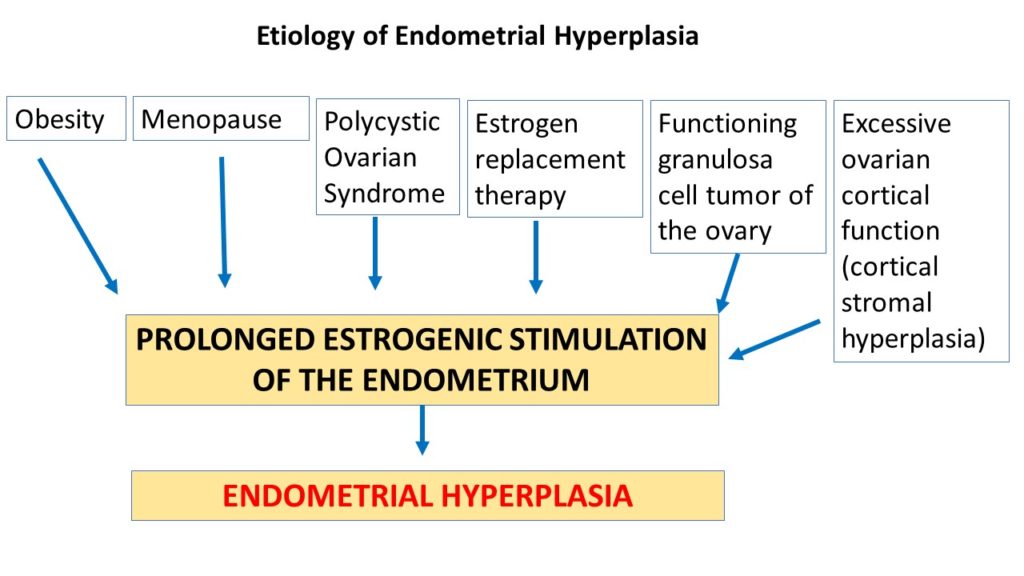
Predominant etiological factor is prolonged estrogenic stimulation of the endometrium as illustrated below
Genetic etiology: seen in 20% of endometrial hyperplasias
• PTEN[Tumor suppressor] gene encodes a lipid phosphatase enzyme which is a negative regulator of phosphatidylinositol 3-kinase (PI3K)/AKT growth-regulatory pathway
• Any mutation of PTEN gene leads to uncontrolled over activity of the PI3/AKT pathway
• This over activity abnormally enhances the ability of estrogen receptors to express its target genes leading to increased and prolonged stimulation by estrogen in turn resulting in Endometrial Hyperplasia
WHO Classification of Endometrial Hyperplasia (2014); is based on morphology;
• Hyperplasia without atypia (Typical Hyperplasia)
• Hyperplasia with atypia (Atypical Hyperplasia)
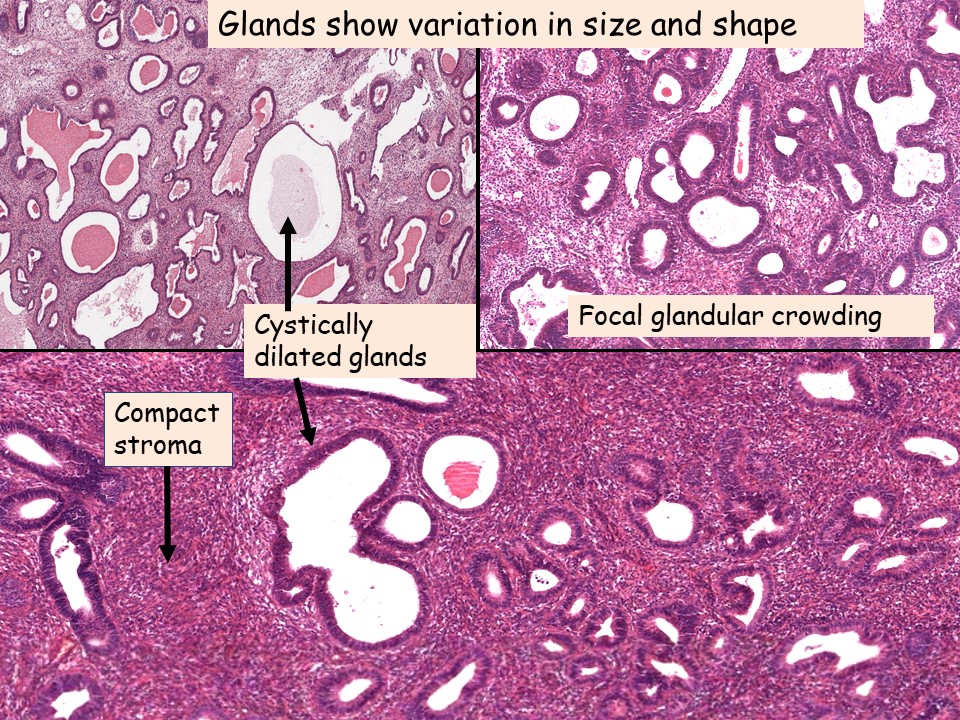
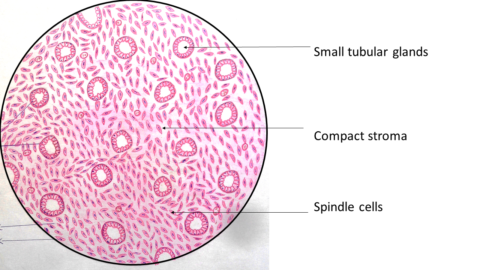
Hyperplasia without atypia (Typical Hyperplasia):
Cardinal feature is increased gland to stromal ratio.
The glands show variation in size and shape, few glands may be cystically dilated.
When the cystically dilated glands are more, those lesions are labeled as cysticoglandular hyperplasia.
Focal glandular crowding may be noted.
Intervening stroma is very much reduced and usually predominantly compact.
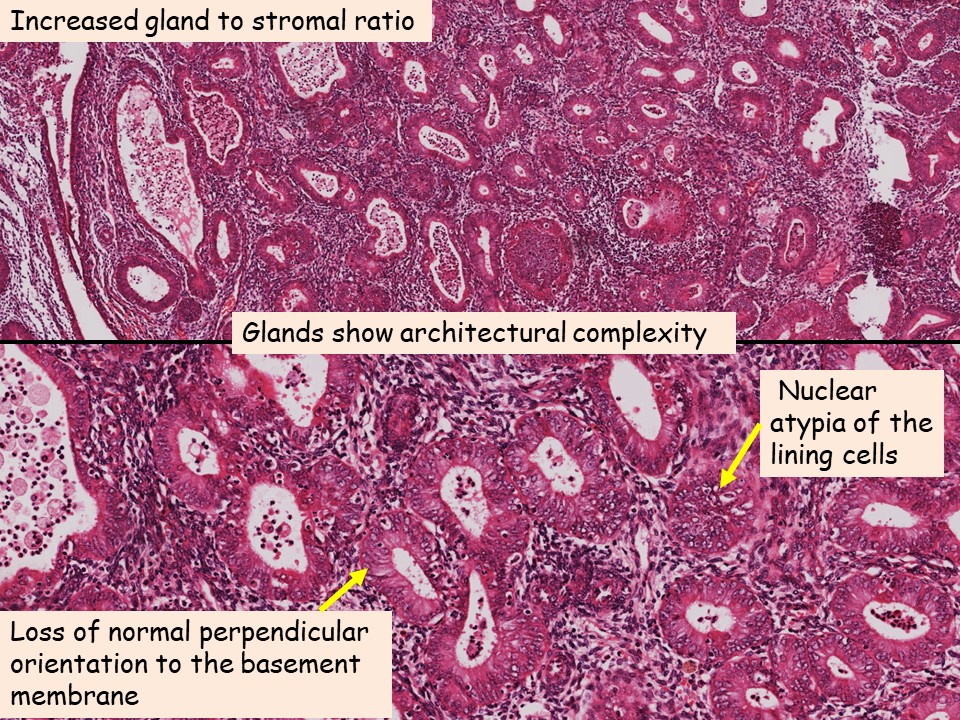
Hyperplasia with atypia (Atypical Hyperplasia):
Increased gland to stromal ratio and these glands show architectural complexity with nuclear atypia of the lining cells. Individual cells are rounded and lose the normal perpendicular orientation to the basement membrane. In addition, the nuclei have open (vesicular) chromatin and conspicuous nucleoli.
Consequences:
• Typical hyperplasia: These lesions are caused by persistent estrogen stimulation and rarely progress to adenocarcinoma (approximately 1% to 3%)
• Atypical hyperplasia: Approximately up to 50% of women are found to have adenocarcinoma on hysterectomy
Treatment:
• Atypical hyperplasia is managed by hysterectomy
• In young women who desire fertility, a trial of progestin therapy with close follow-up is done




{kind=link}
Recent Comments