
CYTOCHEMICAL STAINS IN HEMATOLOGICAL NEOPLASMS.
Author: Dr Faheema Hasan, MD Pathology
cytochemical stains are the special stains that can be performed on peripheral blood smears and bone marrow smears. They play a very important role in diagnosis, differentiation and classification of Leukemias.
These stains can be
1) cytochemical stains ie they use cellular enzymatic reactions to impart staining
or
2) Immunocytochemical stains ie they identify cell specific antigens with the help of antibodies.
Not every lab is equipped with cytogenetics or immunophenotyping. And in that case cytochemical stains can be of immense help in identifying the lineage of the neoplasm.
Let us discuss the various cytochemical stains used in hematology especially in a low resource set up.
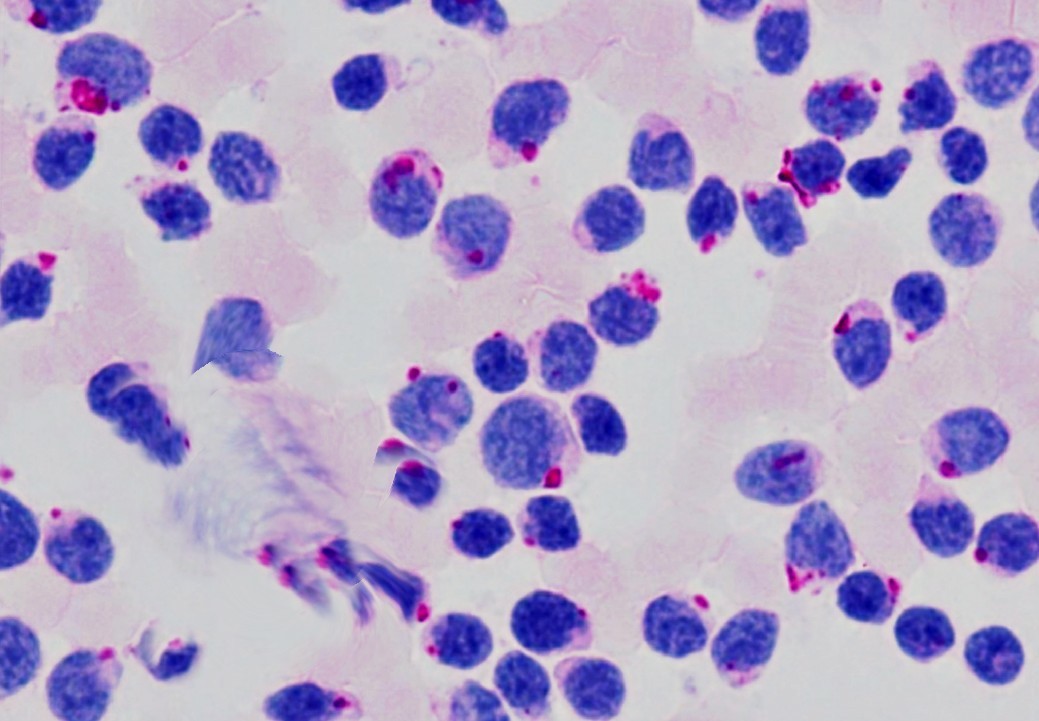
1. Leucocyte alkaline phosphatase (Neutrophil Alkaline Phosphatase)
Alkaline phosphatase activity is present in varying degrees in the cytoplasm of neutrophil , eosinophils, osteoblasts, B lymphocytes and endothelial cells. This activity can be quantified by scoring from 0 to 4+ based on the intensity of the staining. The cell that doesn’t stain is given a core of zero and that has strong staining is given a score of 4. The total score is calculated counting the individual score of 100 neutrophils or bands. Normal LAP score ranges from 15 to 130.
The main utility of LAP score is in differentiating Chronic myeloid leukemia from leukaemoid reaction as both will show a left shift with increased precursors. While leukaemoid reaction will show increased LAP score, it is very low in CML.
Increased Leucocyte alkaline phosphatase is seen in
leukemoid reaction, pregnancy or Oral Contraceptive pills intake , all myeloproliferative disorders except Chronic myeloid leukemia, infections , growth factor therapy, Hodgkin disease etc.
Decreased Leucocyte alkaline phosphatase is seen in
Chronic Myeloid Leukemia, Paroxysmal nocturnal hemoglobinuria, myelodysplastic syndromes, hereditary hypophosphatemia, sickle cell anemia.
NOTE : Collect fresh capillary blood or samples anticoagulated with heparin as there is rapid loss of alkaline phosphatase activity in EDTA vials.
The top neutrophil in this image is a 3+ while the second neutrophil would be scored as a 4+ i.e. the nucleus obscured due to intense cytoplasmic staining. CLICK HERE to access the source of the above image
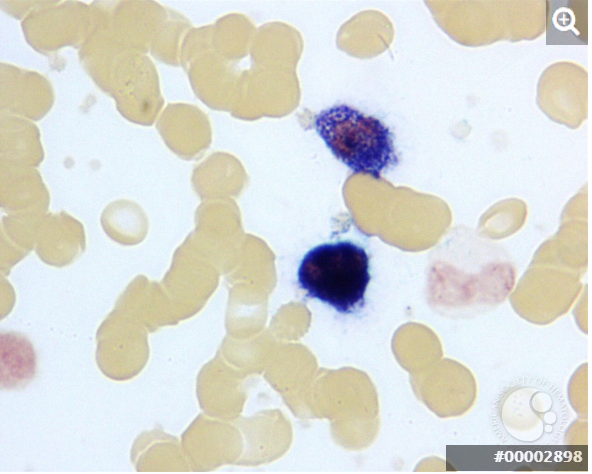
2. Myeloperoxidase stain:
Myeloperoxidase is a component of primary granules of neutrophils. Monocytes are faintly positive while lymphocytes and red blood cells lack the enzyme. This stain is particularly useful in a setting of acute leukaemia, where positive staining indicates that the leukaemic cells are of myeloid origin. The staining depends on the oxidation of Benzidine derivatives by hydrogen peroxide but owing to its potential carcinogenicity, alternative substrates like 3-amino-9-ethyl carbazole or 4-chloro-1-naphthol are being used these days.
But the point to remember are that MPO enzyme is sensitive to light and heat and hence the stain should be performed immediately or protected from light and heat.
There are immunocytochemical stains available for MPO as well.
AML: M3-variant with t(15;17). Very strong myeloperoxidase stain in all cells. Auer rods are not visualized. × 1000.
CLICK HERE to view the source of the above image
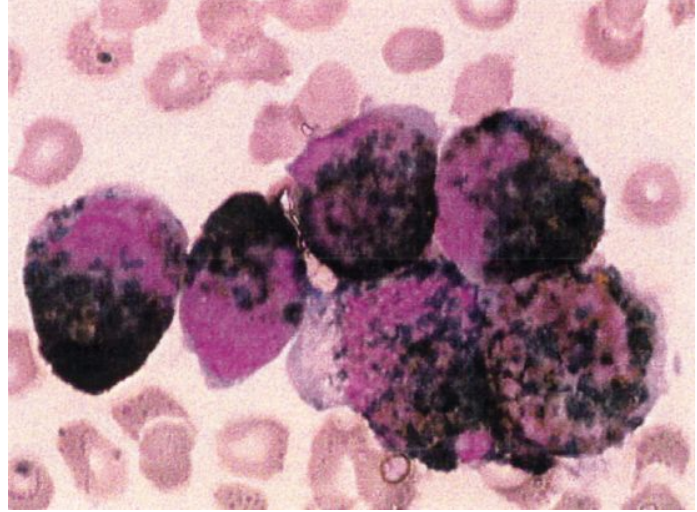
3. Sudan Black B(SBB):
This stain is similar to myeloperoxidase in the lineage it stains, ie it is positive for granulocytes, eosinophils and only weakly in monocytes. But the basis of the stain is not enzymatic, unlike MPO. SBB stains intracellular lipids and phospholipids which are seen in the cells of myeloid lineage and absent or sparse in the lymphoid lineage and hence can be used to identify the lineage of the blasts. However, the blasts of Burkitt’s lymphoma or ALL-L3 may show positive staining in the cytoplasmic vacuoles.
Acute Myeloid Leukemia with Sudan Black B positivity. CLICK HERE to view the source of the above image
4.Esterases:
There are two types of esterases , specific and non specific.
The specific esterase is naphthol AS-D chloroacetate esterase (CAE). These identify the cells of the granulocytic series. It does not stain lymphocytes and monocytes. It can even be used to identify granulocytes in formalin fixed tissues.
The non specific esterase activity is seen in monocytes. Both α-naphthyl butyrate or α-naphthyl acetate can used. The cells of granulocytic series are negative with this stain. The α-naphthyl butyrate stain more specific, while the α-naphthyl acetate stain is more sensitive.
In a suspected myeloid leukemia, dual esterase stains can be used as they can simultaneous classify the blasts as either myeloblasts or monoblasts. Monocytic non specific esterase is Fluoride sensitive.
5. Periodic Acid-Schiff
The periodic acid-Schiff (PAS) stain indicates the presence of intracellular glycogen and neutral mucopolysaccharides.
Cells of many series are positive for PAS, however the staining pattern differs. Erythroleukemias ie AML M6 blasts show an intense diffuse cytoplasmic positivity with PAS, while lymphoblasts show block positivity.
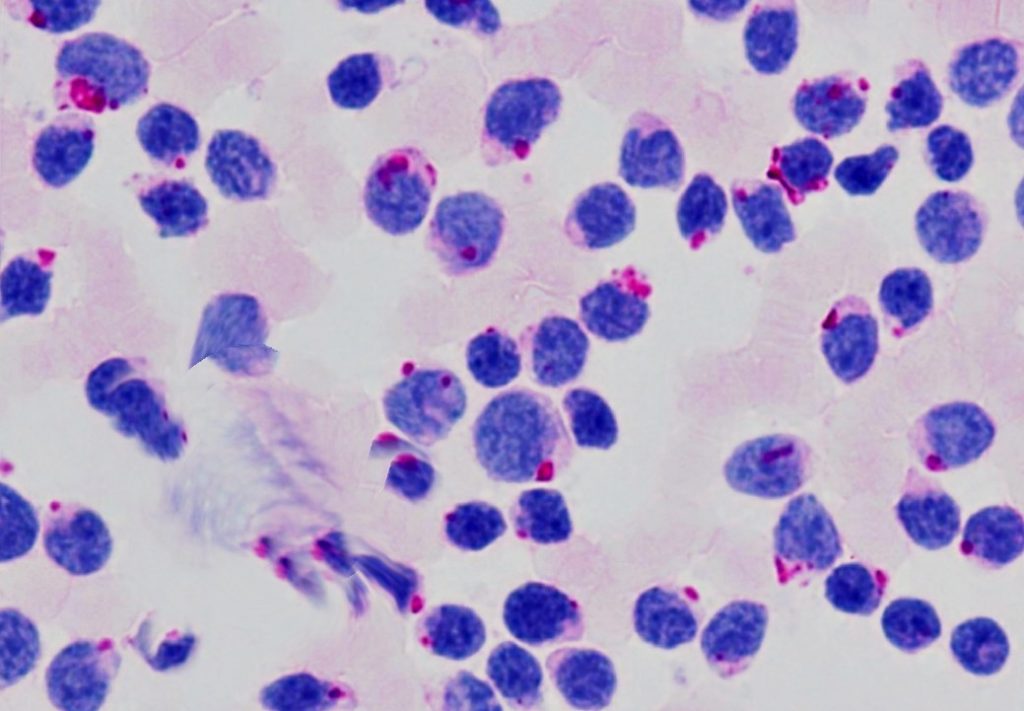
Block positivity for PAS in ALL-L2
6. Toluidine Blue:
Toluidine blue reacts with the acid mucopolysaccharides in the granules of basophils and mast cells to form metachromatic complexes, however, malignant basophils or mast cells may not show a positive reaction.
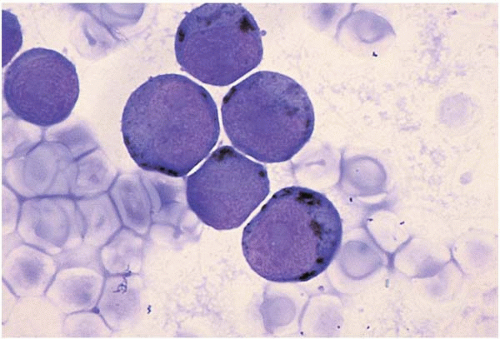
7. Acid Phosphatase
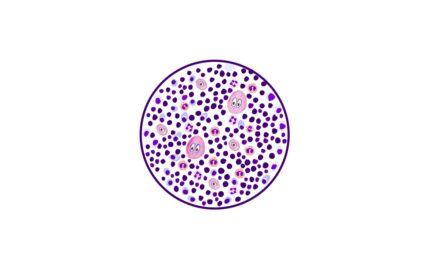
Acid phosphatase is found in all hematopoietic cells, but macrophages have the highest concentration. ‘Dot’like positivity is seen in T lymphoblasts. But in all these cells, acid phosphatase activity is inhibited by tartrate with the exception of hairy cells of Hairy cell leukemia.Hence this property is utilized to diagnose Hairy cell leukaemia.
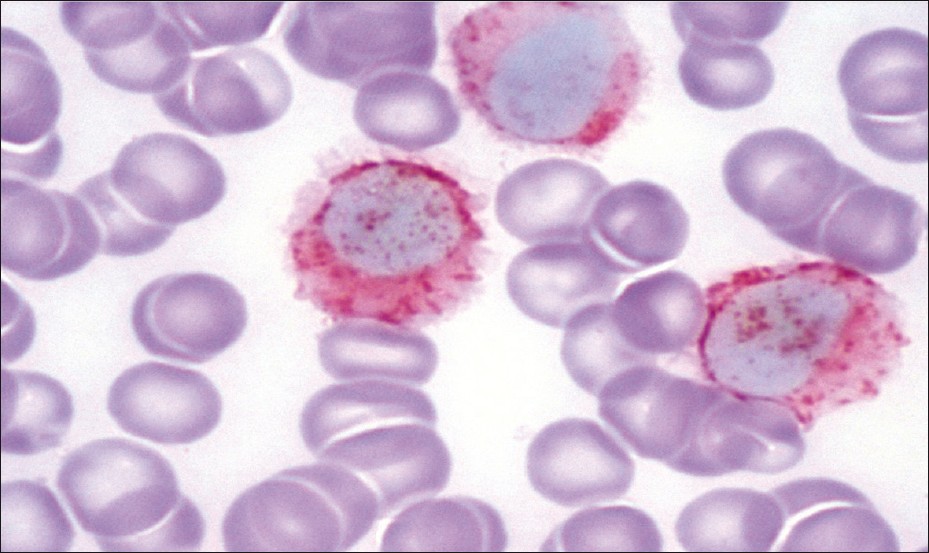
TRAP stain of HCL showing bright granular cytoplasmic positivity in the leukemic cells. (tartrate-treated acid phosphatase stain, ×1000) CLICK HERE to view the source and access to the manuscript
While cytochemical stains may not be in vogue, these stains may be of immense help in a resource poor set up where facilities for immunophenotyping in case of acute leukemia may not be feasible.
Let us have a glimpse of the staining patterns of myeloblasts vs lymphoblasts.
| STAIN | MYELOBLAST | LYMPHOBLAST |
| MYELOPEROXIDASE | Positive | Negative |
| SPECIFIC ESTERASE (CAE) | Positive | Negative |
| SUDAN BLACK B | Positive | Negative |
| PERIODIC ACID SCHIFF | Variable | Block positivity |
| ACID PHOSPHATASE | Negative | Positive in t lymphoblasts |




{kind=link}
Recent Comments